
Remember me

The study protocol was approved by the Institutional Ethics Committee of the Faculty of Medicine and Dentistry, Palacky University Olomouc and Olomouc University Hospital. Ethics approval for this study was granted in accordance with the Olomouc University Hospital standard SM-L031, and the ethics committee reference number is 88/21. All patients and healthy controls were informed about the purpose and the design of the study and they all signed informed consent forms. Patient enrollment, data collection, sampling, and laboratory examinations took place between 2022 and 2025. No blinding was performed.
Disease classification was based exclusively on clinically established diagnoses, as pathological confirmation was not feasible due to the use of skin biopsies obtained from living subjects. All diagnoses were determined by experienced neurologists according to currently accepted clinical diagnostic criteria for the respective disorders. The terms “confirmed α-synucleinopathy” and “confirmed tauopathy” therefore refer to clinically confirmed diagnoses and do not imply neuropathological verification.
The patient samples (120) were divided into groups according to diagnoses established using current validated and updated clinical criteria (Alexander et al. 2014; Armstrong et al. 2013; Bhidayasiri et al. 2019; Boxer et al. 2017; Gilman et al. 2008; Höglinger et al. 2017; McKeith et al. 2020; Postuma et al. 2015). Patients were included in the study if they were able to undergo all examinations specified in the study protocol, complied with follow-up visits, and had no serious comorbidities that could interfere with the planned assessments, such as cancer, hematological disorders, depression, or psychosis. The patients diagnosed with proteinopathy were divided into groups based on their clinical diagnoses and clinical-pathological taxonomy:
1)parkinsonian syndromes (Park.sy.) (patients without a confirmed clinical diagnosis; the disease may develop either on the side of α-synucleinopathies or tauopathies) (the cohort contained 33 patients);
2)α-synucleinopathies group (idiopathic Parkinson´s disease (IPD), Parkinson´s disease (PD), Lewy body disease (LBD) (the cohort contained 53 patients);
3)multiple system atrophy (MSA) group (the cohort contained 6 patients);
4)tauopathies group (progressive supranuclear palsy (PSP), corticobasal degeneration (CBD), frontotemporal dementia (FTD) (the cohort contained 16 patients);
5)other diagnoses group (including restless legs syndrome, polyneuropathies, hypokinetic-rigid syndrome, dopamine transporter deficiency) (the cohort contained 12 patients) and compared with 6) control group (HC) (vertebrogenic-algic syndrome, lumboischiadic syndrome) (the cohort contained 20 patients). The exclusion criteria for HC were the presence of neurodegenerative disease (in the patient or family history) or peripheral polyneuropathy.
We analyzed 58 male and 62 female patient samples. The average age of the patients was 67 years. The HC consisted of 13 males and 7 females samples. The average age of HC was 70 years (Table 1).
Table 1 Demographic and clinical characteristics of study cohortsSkin BiopsySample Collection and ProcessingPrior to the outpatient excision biopsy using a circular scalpel (Fig. 2), local anesthesia was administered - typically 1% Mesocaine (alternative anesthetics were used in patients with Mesocaine allergy). The anesthetic was applied to the soft tissues (skin and subcutaneous tissue) at the biopsy sites on the back and the distal leg. No side effects of the biopsy procedure were reported.
The collected samples were then immersed in 4% paraformaldehyde and fixed for 4 h at room temperature. Then, the samples were placed in a buffer consisting of 10% sucrose in phosphate buffer for 24 h at a temperature of 2–4 °C. The next day, the samples were removed from the solution and immediately cut into Sect. 50 and 20 μm thick using a cryostat microtome (Leica CM1950, Leica Biosystems). The sections were cut directly onto glass microscope slides and were not processed as free-floating sections. The sections were then left to dry for 24 h on a plate at laboratory temperature. Then, they were transferred to an incubator (JOUAN, Innovens) where they were dried at a temperature of 47 °C. Finally, the slides were stored in histology boxes in a freezer at -20 °C until further immunohistochemical or immunofluorescence staining. All staining, incubation, washing, and mounting procedures were performed directly on the slides, using a coverslip and mounting medium for final preservation of the tissue sections.
Fig. 2
Skin punch biopsy procedure and evaluation workflow. Schematic representation of skin biopsies with a circular scalpel. In skin biopsies, after processing, we evaluated the quantitative amount of IENFD in the epidermis and the qualitative presence of p-α-syn in all skin layers. The image was created using AI-Gemini, an advanced AI-powered image creation tool
Fluorescent StainingPrior to incubation with fluorescent staining, the sections were slowly thawed at room temperature. Primary antibody incubation was performed as follows: the samples were fixed in 100% acetone: methanol at -20 °C for 10 min, rinsed with water for 5 min, and subsequently washed in phosphate-buffered saline containing 0.3% bovine serum albumine and 0.1% Tween 20 for 10 min. Afterwards, the slides were incubated with 3% normal goat serum for 30 min without further rinsing. Primary antibodies (raised in mouse) were then applied, mixed into a single tube, and diluted in the primary antibody diluent: PGP 9.5 (ThermoFisher Scientific), dilution 1:100 and purified anti-α-Synuclein phospho (Ser129) antibody (BioLegend), dilution 1:50. The sections were incubated with the primary antibody solution for 20 h at room temperature. Secondary antibody incubation followed rinsing in PBS (3 × 5 min) to remove residual primary antibodies. Secondary antibodies were mixed into one tube and diluted in the secondary antibody diluent: fluorescein isothiocynate-conjungate antibody (Millipore), dilution 1:100 and DyLight 550- conjungated antibody (ThermoFisher Scientific), dilution 1:500. The slides were incubated with the secondary antibody solution for 1 h at room temperature in the dark, rinsed in PBS (2 × 5 min), and finally rinsed with distilled water. The samples were then mounted in Mowiol mounting medium (Altium International).
The slides were evaluated using indirect immunohistochemistry at 200x magnification under a microscope (Olympus BX40, Olympus Corporation) with a fluorescent lamp (Olympus U-RFL-T, Olympus Corporation). The Olympus cellSens Standard program was used to evaluate and record the microscopic evaluation results.
The following features were evaluated: (1) the presence of p-α-syn in all layers of the skin – i.e. the epidermis, subepidermal tissue, and dermis. The evaluation was qualitative, with a yes/no (present/absent) result; (2) the density of thin fibers in the epidermis, with the result being the average number of thin fibers per length of epidermis.
According to the guidelines of the European Federation of Neurological Societies, PGP 9.5 positive nerve fibers at the epidermis-dermis junction were counted manually, and the length of the epidermal basement membrane was measured to calculate the intraepidermal nerve fiber density (IENFD; fibers/mm) (Lauria et al. 2010).
All samples were evaluated as standardized sections of 50 μm, as well as optimized sections of 20 μm thickness (Fig. 3). ImageJ software was used to evaluate and merge individual images.
Fig. 3
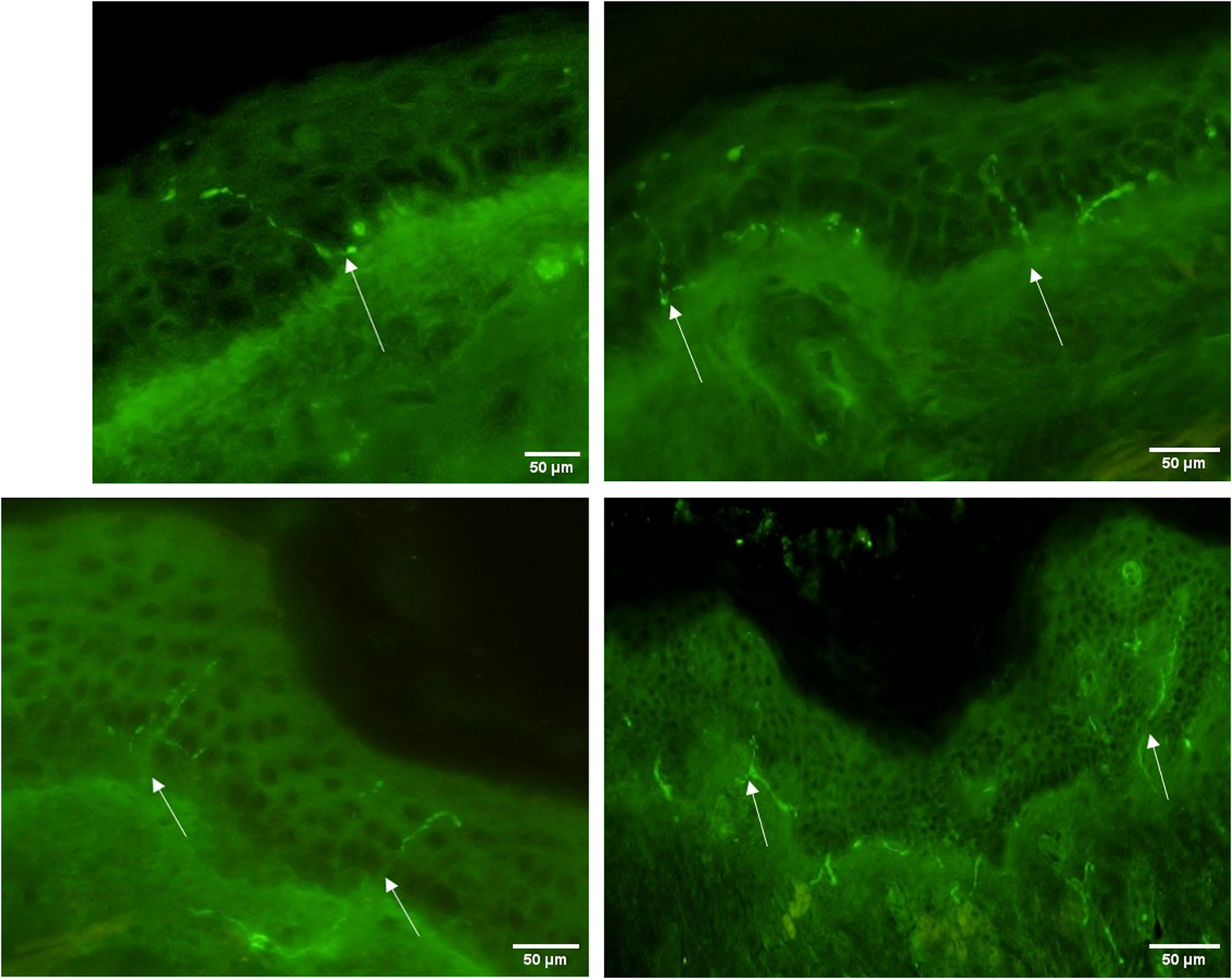
Cutaneous p-α-synuclein deposit detected by double immunofluorescence. Microscopic images of p-α-syn (marked with white arrows). The positive fibers present follow the course of the fiber and show very clear staining. The scale is 50 μm and the magnification is 200x. In most cases, the presence of p-α-syn is recorded only in the dermis, less frequently in the subepidermal space, and very rarely in the epidermis.s detected by double immunofluorescence
Evaluation of the Presence of p-α-synThe presence of p-α-syn was evaluated in all samples, both from the leg and the back.
Evaluation of IENFD PresenceThe presence of IENFD was evaluated in leg samples with a slice thickness of 20 μm.
IENFD quantification was performed manually according to internationally accepted morphological criteria to ensure consistent identification of intraepidermal nerve fibers. In the microscopic field, the presence of IENFD was determined using the following rules:
1.Only nerves passing through the basement membrane into the epidermis are counted;
2.Nerves that branch before passing through the basement membrane are counted as two fibers;
3.Nerves that branch in the basement membrane are counted as two fibers;
4.Nerves that branch after crossing the basement membrane are counted as one fiber;
5.Fragments of nerves that pass through the basement membrane are counted;
6.Nerve fibers that approach the basement membrane but do not pass through it are not counted;
7.Epidermal nerve fragments that do not pass through the basement membrane are not counted (Fig. 4) (Bakkers et al. 2009).
These criteria ensured standardized fiber discrimination and minimized counting variability across samples.
IENFD was evaluated quantitatively in all skin biopsy samples according to established criteria. Individual nerve fiber counts were obtained for each patient and used for subsequent statistical analyses, including assessment of relationships with age and disease duration. For group-wise comparisons, IENFD results were additionally categorized as preserved or reduced, and the presence or absence of IENFD reduction was used for statistical evaluation across diagnostic groups.
Fig. 4
Principles of IENFD fiber counting. Principles of IENFD fiber counting
Evaluation of Olfactory Test ResultsAll patients and control group participants underwent a series of olfactory tests consisting of 12 synthetic odors (Screening 12 Test CZ LA-13-00001, MediSense). These tests were used to determine the preclinical development of neurodegenerative processes. The results of the olfactory tests were scaled as follows: 0 ≥ 6 correct answers correspond to anosmia, 6–10 to hyposmia, and 10 ≤ 12 to normosmia (Graph 1).
Graph 1
Olfactory performance in patient groups and controls. Graph illustrating the distribution ofanosmia, hyposmia, and normosmia in healthy controls and patient groups. Anosmia wassignificantly more frequent in parkinsonian syndromes, IPD + PD + LBD, and tauopathiescompared to controls
Comments (0)