Due to its clinical characteristics of high aggressiveness and a tendency to have multiple metastases, HER2-positive breast cancer (HER2 + BC) has always been regarded as a single breast cancer subtype and treated accordingly [18]. Among patients with HER2 + BC, those with HER2 + BC-LM had a very poor prognosis. Stratifying patients according to prognosis and predicting the prognosis of patients with HER2 + BC-LM remain a challenge for clinicians, despite the great efforts made by researcher [19, 20]. Thus, it is necessary to predict the survival of patients with HER2 + BC-LM based on a clinical model of a large population. Thus, in our study, we developed a prognostic nomogram for predicting the OS of patients with HER2 + BC-LM at 6 months, 1 year, and 2 years through the training cohort. Moreover, our model was validated in the validation cohort and showed acceptable accuracy in predicting the OS of patients with HER2 + BC-LM. Our model, although not introducing novel predictors, enables individualized prognosis estimation for HER2 + BC-LM patients based on real-world data, aiding clinical decision-making especially where treatment options are limited.
It was found through univariate Cox regression analysis that marital status was a factor related to the prognosis of patients with HER2 + BC-LM. This may be affected by the economic and psychosocial variables. Patients who are divorced, widowed, or separated lack the support and care from their spouses and often have a poor mental state and bad lifestyle habits (e.g., smoking and excessive drinking), which lead to the development of tumors and insufficient treatment of diseases [21, 22]. In contrast, the more stable economic support provided by spouses or partners of married patients may be an important reason for patients to better receive surgeries and adhere to adjuvant treatments [23]. In terms of psychosocial aspects, single patients face more pain, depression, and anxiety due to the lack of companionship and comfort [24], and these negative emotions are all regarded as factors that can facilitate tumor progression and affect treatment outcomes [25]. Interestingly, our study revealed that marital status can predict prognosis in univariate analysis, but it is not an independent predictor of prognosis in multivariate analysis.However, as a significant proxy for social support, the prognostic value of marital status has been confirmed in multiple studies. Married patients generally possess greater psychological resilience, better treatment adherence, and more abundant family caregiving resources, all of which may indirectly contribute to improved survival outcomes. Although in the multivariate co-linearity context of this study (or in association with other significant variables such as ECOG performance status and age), the independent effect of marital status was diluted (P > 0.05), the importance of the “social support” it represents cannot be overlooked in the long-term management of cancer patients.In conclusion, although marital status is associated with prognosis in univariate analysis or clinical context, multivariate models have not confirmed its independent prognostic value. Therefore, marital status is only included as an auxiliary predictor in clinical decision-making.
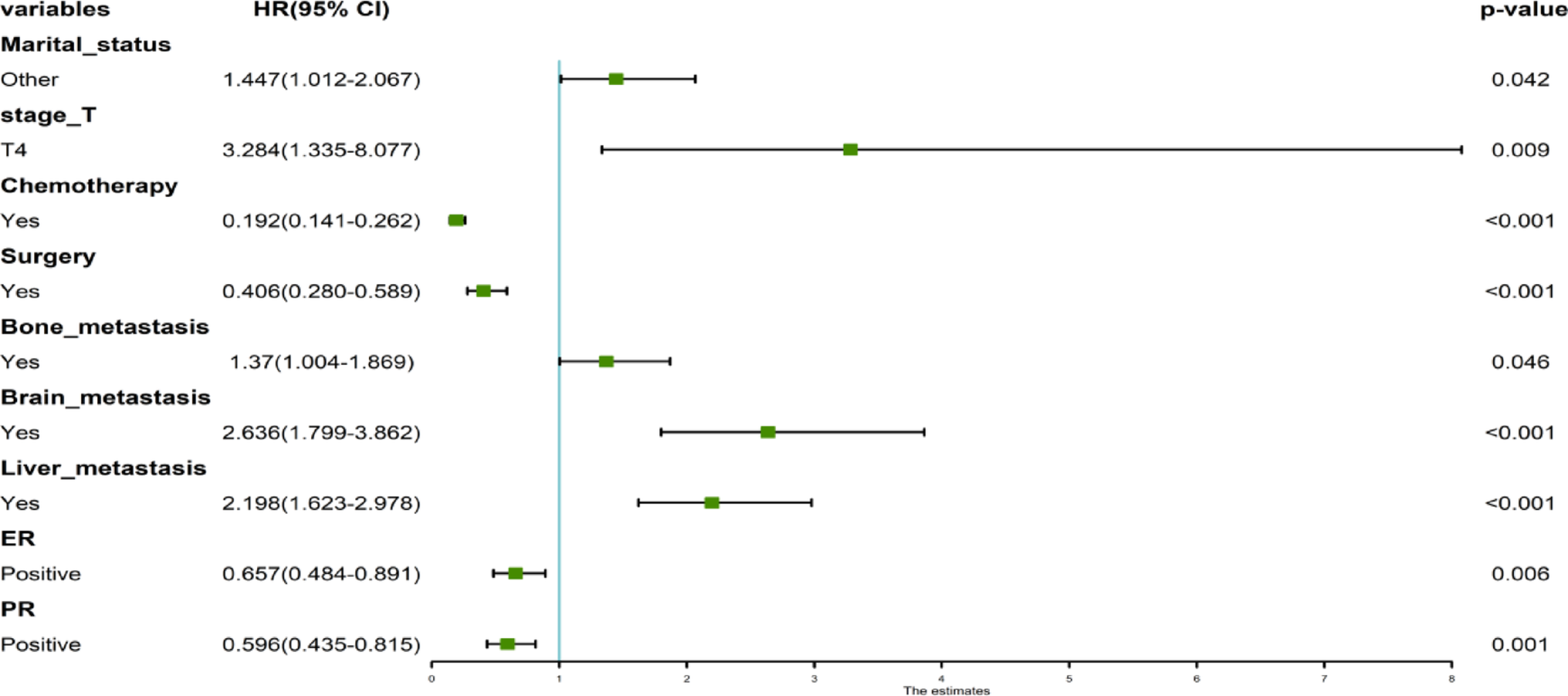
The multivariate Cox regression analysis revealed that a larger primary tumor (T4 Stage), extrapulmonary metastases (including liver and brain metastases), surgery and systemic chemotherapy, ER, and PR were significantly correlated with a better prognosis for patients with HER2 + BC-LM and were independent prognostic factors. It has been found that a larger primary tumor (T4 Stage) is related to a poorer prognosis for patients with HER2 + B-LM. Among patients with MBC with a poorer prognosis, patients with a larger primary tumor often have a higher KAM score, which indicates a poorer OS [26]. Thus, they are more likely to undergo more aggressive systemic treatments (e.g., chemotherapy) after being diagnosed with lung metastasis.The independent inclusion of ER+ (HR = 0.630, p = 0.016) and PR+ (HR = 0.631, p = 0.015)in the multivariate analysis raises concerns about collinearity, as these receptors are highly correlated, potentially affecting model stability.But retained both ER + and PR+ independently in the final model to dissect their individual contributions to survival outcomes, supported by prior evidence of distinct biological roles in tumor progression.However, it should be noted that although the independent inclusion of ER and PR is based on their biological mechanisms, the two are usually highly correlated in clinical data. Due to the lack of expression levels for ER and PR in the SEER database, this study did not calculate the variance inflation factor (VIF) or conduct a combination variable analysis to quantify the degree of collinearity. Therefore, the independent interpretation of ER + and PR+coefficients needs to be carefully understood in conjunction with clinical background, and future research should be further validated through more refined receptor data.
Extrapulmonary metastases (including bone, liver, and brain metastases) were also found to be an independent prognostic variable. HER2 + BC patients with more organ metastases have a heavier tumor burden and greater tumor heterogeneity and are more likely to develop treatment resistance. Interestingly, according to the multivariate Cox regression analysis, the bone metastases were no longer significant, which might be attributed to the sample size.However, bone metastasis as a common metastatic site in advanced disease, its presence is often associated with higher tumor burden, poorer performance status (e.g., higher ECOG score), and a more complex risk of complications. In the present model, bone metastasis may be correlated with significant variables such as disease stage and pain management (e.g., patients with bone metastasis are more likely to be at an advanced stage and receiving palliative care), which could obscure its direct effect.In summary, although marital status and bone metastasis are not independent prognostic drivers, they serve as key descriptors of individual patient characteristics and disease status, only included as auxiliary variables in the model, to enhancing the model´s ability to capture real-world heterogeneity.
In terms of treatment, we found that the survival period of patients with HER2 + BC-LM who received palliative surgery or systemic chemotherapy was significantly prolonged (measured in months), while no difference in radiotherapy was observed. Previously, because MBC was regarded as an incurable disease, the aim of treating these patients was to provide relief through systemic treatment. Breast surgery was only performed when the tumor was symptomatic. It was not until recently that people believed that once distant metastases occurred, (aggressive) local treatment would not offer a survival advantage and should not be an option for treatment. However, some retrospective studies have suggested that patients with primary distant MBC may benefit from the resection of breast tumors [27]. A recent prospective clinical trial reported that among patients with MBC who underwent surgical resection of the primary tumor at the initial diagnosis, compared with those who did not receive surgical resection of the primary tumor, their risk of death was reduced by 34%, and the 5-year OS rate was increased by 17.2% [28]. Moreover, a large-scale meta-analysis of multiple retrospective studies has shown that patients with breast cancer lung metastasis may achieve a significantly better prognosis after resection of the primary tumor [29, 30]. Moreover, in our study, chemotherapy was significantly associated with the improvement of OS in patients with HER2 + BC-LM. According to the latest clinical guidelines, chemotherapy, including that for BC-LM, remains the fundamental treatment method for MBC [31]. Furthermore, studies have shown that the combination of pertuzumab, trastuzumab (targeted therapies), and docetaxel (chemotherapy) is the standard treatment regimen for the first-line treatment of HER2 + MBC, and this treatment is associated with better survival rates in patients with HER2 + MBC [32]. Therefore, future studies should investigate the appropriate chemotherapeutic drugs and optimize chemotherapy strategies to improve the prognosis of HER2 + BC-LM patients. Moreover, in our study, the positivity of the ER and PR was also significantly associated with the improvement of OS in the HER2 + BC-LM patients. Because endocrine sensitivity is directly related to the positive degree of hormone receptors, endocrine treatment is a standard treatment method for breast cancer. International guidelines recommend endocrine treatment as the first-line treatment option for patients with hormone receptor-positive MBC [33]. One study reported that in MBC with both hormone receptor positivity and HER2-positive status, especially when the disease burden is limited and there is no visceral crisis, the combined use of endocrine treatment and anti-HER2 treatment is an acceptable approach [34].
This article established a model to predict the prognosis of the HER2 + BC-LM patients by utilizing the important variables determined through Cox regression analysis. To evaluate the predictive ability of our model, the C-index and generated calibration plots were calculated. In the training group and the internal validation group, the C-index values of our prognostic nomogram were 0.813 and 0.787, respectively. According to previous studies, a nomogram with a C-index exceeding 0.7 is considered to have satisfactory sensitivity and specificity [35]. Moreover, the reliability of our nomogram was evident from the calibration curves, which indicated a very good fit between the predicted results and the observed results in both cohorts. Therefore, the model established in this study performed well in predicting the survival of the HER2 + BC-LM patients. This is a rare study aiming to simultaneously improve the prognosis of the HER2 + BC-LM patients, and we hope that this model can assist in risk stratification and clinical decision-making.Compared to previous studies, the nomogram developed in the present study incorporates treatment variables such as surgery, chemotherapy, and radiotherapy. In contrast, the model by Lyu et al. [36] only included clinicopathological features, while the model by Chen et al. [37] did not account for radiotherapy. This difference enables our model to more comprehensively reflect the actual treatment profile of patients.
However, this study has several limitations. First, this study is retrospective and inherently carries some unavoidable biases. Second, Unadjusted survival analysis revealed apparent differences between treatment groups: patients receiving surgery had a median survival of > 40 months compared to 18.5 months in the non-surgical group (P < 0.001), while those receiving chemotherapy had > 40 months versus 6.5 months in the non-chemotherapy group (P < 0.001). These striking disparities, however, likely reflect significant treatment selection bias-where healthier patients with inherently better prognoses were more likely to receive surgery or chemotherapy-rather than the true causal effect of interventions. These results are presented solely as unadjusted descriptive findings and should not be interpreted as treatment efficacy estimates.Third, clinicopathological factors (e.g., the expression levels of CK5/6, ki−67, p53, etc.) may affect the survival outcomes of HER2 + BC-LM patients and are worthy of our consideration in future studies. Unfortunately, these crucial details could not be found in the SEER database, thus limiting their inclusion in our current model. However, the impact of these factors on the prognosis of the HER2 + BC-LM patients merits further investigation. Fourth, more detailed treatment information could not be obtained from the SEER database. In particular, a trend toward precision and individualized treatment for cancer patients, including the timing and regimens of various treatments, can be observed. The present study is a clinical trial, and the mechanism has not yet been further explored. Therefore, more efforts are needed in the experimental research.

Comments (0)