
Remember me
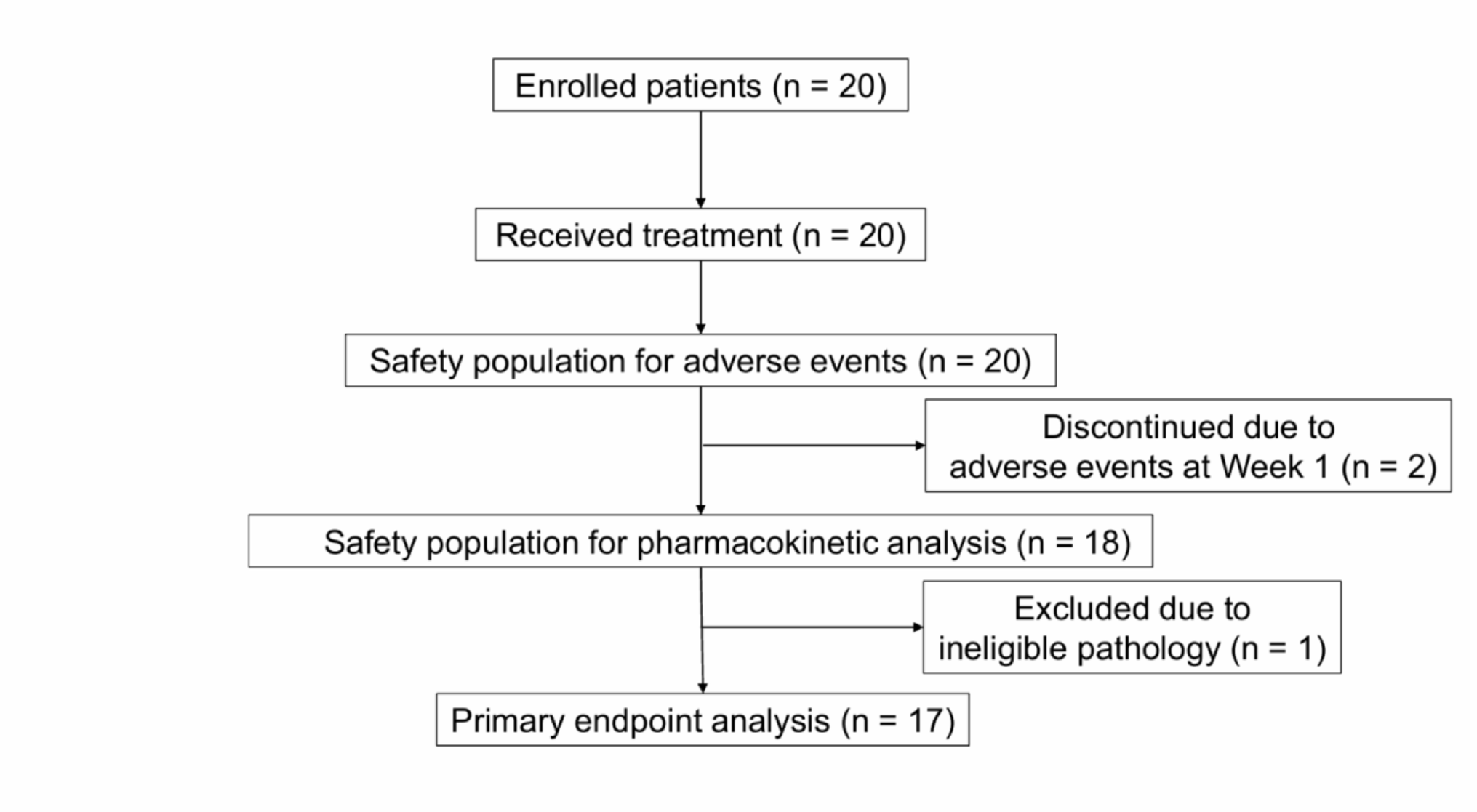
A total of 693 patients were enrolled in the P-BRIDGE study and were included in the present analysis, including 426 patients who received palbociclib plus ET as 1L and 267 patients who received palbociclib plus ET as 2L treatment (Fig. S1).
Among 1L patients, 266 (62.4%) were aged < 65 years, 118 (27.7%) were aged ≥ 65 to < 75 years, and 42 (9.9%) were aged ≥ 75 years. Among 2L patients, 161 (60.3%) were aged < 65 years, 66 (24.7%) were aged ≥ 65 to < 75 years, and 40 (15.0%) were aged ≥ 75 years. Of those aged ≥ 75 years, 11 in the 1L setting and 15 in the 2L setting were aged ≥ 80 years.
Demographic and clinical characteristics of patients receiving palbociclib plus ET as 1L and 2L treatment according to age group are presented in Table 1. In both the 1L and 2L treatment groups, the proportion of patients with comorbidities at the time of palbociclib initiation tended to increase with age. The proportion of patients with cardiac disease was highest in the ≥ 75-year age group in both the 1L and 2L treatment groups. In the 1L treatment group, the proportion of patients with bone metastases only, those with a treatment-free interval (TFI) < 12 months, and pre- and post-operative ET and CT decreased with increasing age. Conversely, the proportion of patients without symptoms at the time of palbociclib initiation increased with age. In the 2L treatment group, the proportion of patients with visceral metastases increased with age, but no other consistent trends were observed.
Table 1 Patient demographics and clinical characteristicsReal-world treatment pattern and dose modification of palbociclib by age group and treatment lineIn the 1L setting, the palbociclib starting dose was 125 mg in 95.5%, 88.1%, and 64.3% of patients aged < 65 years, ≥ 65 to < 75 years, and ≥ 75 years, respectively (Table 2). There were no relevant differences across age groups in the 2L setting.
Table 2 Treatment patterns and dose modifications of palbociclibThe rate of dose reductions was similar between age groups in the 1L setting (< 65 years: 75.2%; ≥ 65 to < 75 years: 75.4%; ≥ 75 years: 66.7%). In the 2L setting, patients aged ≥ 65 to < 75 years were most likely to experience dose reductions (81.8%) followed by those aged ≥ 75 years (72.5%) and < 65 years (65.8%).
The overall treatment discontinuation rate was slightly higher in patients aged ≥ 65 to < 75 years (82.2%) and ≥ 75 years (85.7%) compared with those aged < 65 years (75.2%) in the 1L setting. In the 1L setting, the most common reason for treatment discontinuation excluding PD was AEs (< 65 years: 11.3%; ≥ 65 to < 75 years: 19.5%; ≥ 75 years: 40.5%), followed by other reasons (< 65 years: 7.1%; ≥ 65 to < 75 years: 11.9%; ≥ 75 years: 14.3%). Overall, patients aged ≥ 75 years in the 1L setting were more likely to discontinue treatment due to AEs compared with other age groups, most commonly due to non-hematologic toxicity. Non-hematologic AEs leading to treatment discontinuation in patients aged ≥ 75 years in the 1L setting were rash (n = 2), decreased appetite (n = 2), interstitial lung disease (n = 1), pulmonary toxicity (n = 2), malaise (n = 1), depression (n = 1), hypoaesthesia (n = 1), palmar-plantar erythrodysaesthesia syndrome (n = 1), and pruritus (n = 1) (Table S1). Notably, in patients aged ≥ 75 years, treatment discontinuation was most common from 9 months after initiation. Discontinuation rates within the first 6 months were consistent across all age groups (Table S2).
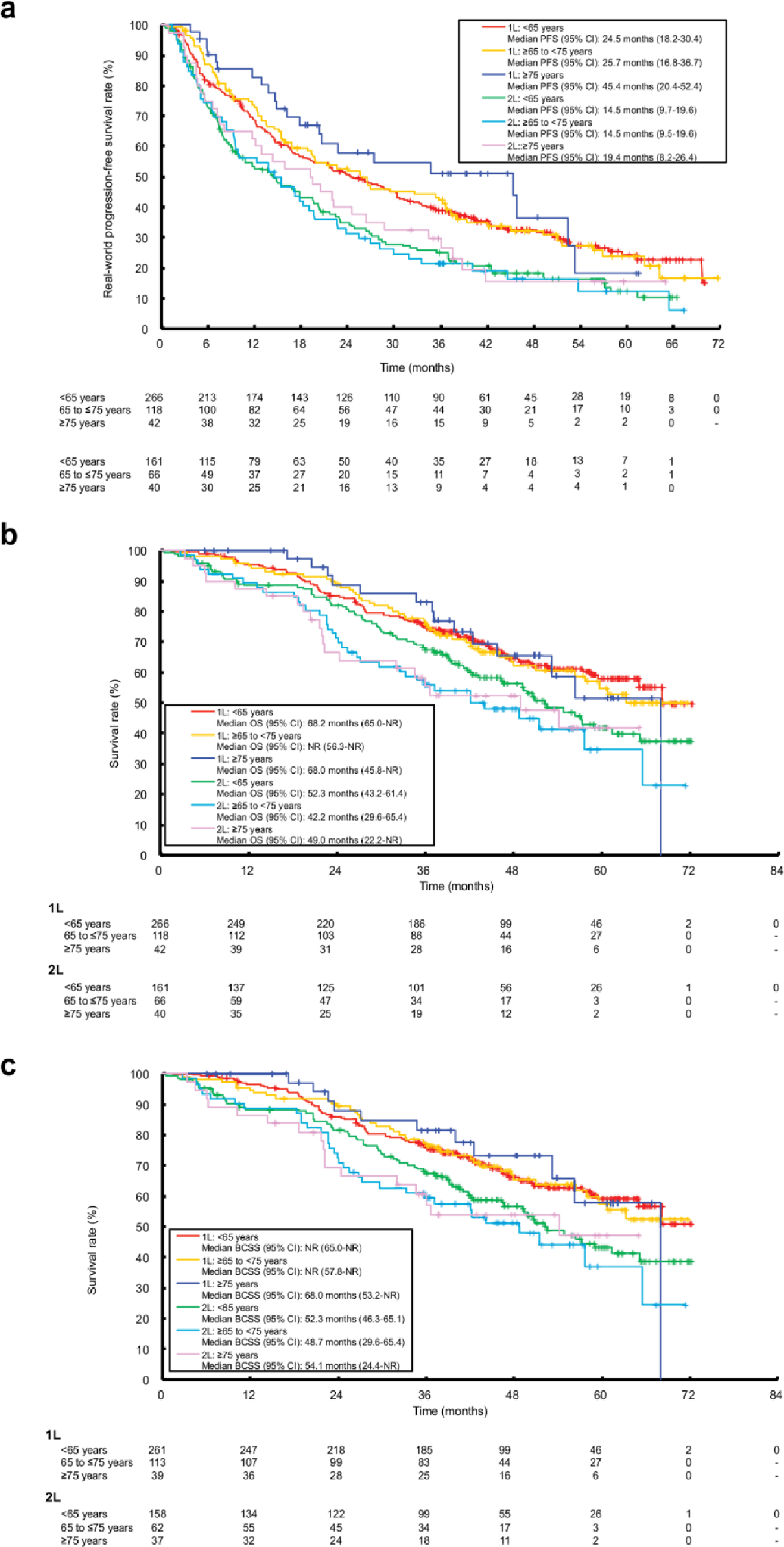
RwPFS, RwCFS and OS by age group and treatment lineThe mean (interquartile range [IQR]) follow-up time in the 1L treatment group from palbociclib initiation was 49.0 months (39.5–59.6) for patients aged < 65 years, 51.1 months (39.0-63.6) for those aged ≥ 65 to < 75 years, and 43.4 months (28.8–52.6) for those aged ≥ 75 years. In the 2L treatment group, corresponding median follow-up times were 48.4 months (38.8–62.1), 46.7 months (40.0–55.6) and 47.9 months (36.6–56.4), respectively. RwPFS, and OS, including overall survival and breast cancer-specific survival, are presented for each age group by treatment line in Fig. 1a–c. In the 1L treatment group, median rwPFS (95% CI) was 24.5 months (18.2–30.4), 25.7 months (16.8–36.7), and 45.4 months (20.4–52.4), in the < 65, ≥ 65 to < 75, and ≥ 75 years groups, respectively (Fig. 1a). In the 2L treatment group, corresponding median rwPFS (95% CI) was 14.5. months (9.7–19.6), 14.5 months (9.5–19.6), and 19.4 months (8.2–26.4), respectively (Fig. 1a).
Fig. 1
Real-world a PFS, b OS (all cause), and c breast cancer-specific survival with palbociclib plus ET as 1L and 2L treatment by treatment line and age group. ET endocrine therapy; OS overall survival; PFS progression-free survival; 1L first line; 2L second line
Patients aged ≥ 75 years who initiated palbociclib treatment in the 1L setting at 125 mg/day tended to show longer median rwPFS (45.8 months, 95%CI: 27.3-NR) compared with those who initiated palbociclib treatment at 100 mg/day or 75 mg/day (20.4 months, 95%CI: 5.9-NR; Fig. 2).
Fig. 2
rwPFS in patients aged ≥ 75 years initiating palbociclib treatment at a starting dose of 125 mg versus 100 mg or 75 mg by treatment line and dose group
Median OS was similar across age groups in the 1L treatment setting, but there was a tendency towards longer OS in patients aged < 65 years in the 2L treatment setting (Fig. 1b). In the 1L treatment group, median OS (95% CI) was 68.2 months (65.0-NR) in patients aged < 65 years, NR (56.3-NR) in patients aged ≥ 65 to < 75 years, and 68.0 months (45.8-NR) in patients aged ≥ 75 years (Fig. 1b). In the 2L treatment group, median OS (95% CI) was 52.3 months (43.2–61.4) in patients aged < 65 years, 42.2 months (29.6–65.4) in patients aged ≥ 65 to < 75 years, and 49.0 (22.2-NR) in patients aged ≥ 75 years (Fig. 1b).
Exploratory analysis showed that median breast-cancer specific survival (95% CI) was similar among patients aged ≥ 75 years (68.1 months [53.2-NR]) and those aged < 65 years (NR [65.0-NR]) and ≥ 65 to < 75 years (NR [57.8-NR]) in the 1L setting, and slightly longer in patients aged ≥ 75 years (54.1 months [24.4-NR]) versus those aged < 65 years (52.3 months [46.3–65.1]) and ≥ 65 to < 75 years (48.7 months [29.6–65.4]) in the 2L setting (Fig. 1c). A total of 154 (36.2%) and 135 (50.6%) deaths occurred in 1L and 2L settings, respectively, with similar rates across age groups (1L, < 65 years: 35.3%; ≥ 65 to < 75 years: 39.0%; ≥ 75 years: 33.3%; 2L, < 65 years: 48.4%; ≥ 65 to < 75 years: 56.1%; ≥ 75 years: 50.0%). In 1L, breast cancer was the cause of death in 89 (94.7%) deaths aged < 65, 41 (89.1%) aged ≥ 65 to < 75, and 11 (78.6%) aged ≥ 75 years; other causes accounted for 1 (1.1%), 3 (6.5%), and 1 (7.1%) deaths, respectively. In 2L, breast cancer caused 75 (96.2%), 33 (89.2%), and 17 (85.0%) deaths in the same age groups; other causes accounted for 2 (2.6%), 4 (10.8%), and 1 (5.0%) deaths, respectively.
RwCFS was similar across all age groups in the 1L and 2L setting (Fig. 3a). Median rwCFS (95% CI) was 36.2 months (30.7–44.5) in patients aged < 65 years, 37.9 months (26.9–57.8) in patients aged ≥ 65 to < 75 years, and 42.5 months (29.4–56.3) in patients aged ≥ 75 years in the 1L setting. In the 2L setting, corresponding median rwCFS was 24.4 months (18.0-28.8), 20.6 months (15.3–26.7), and 24.5 months (19.5–39.3), respectively.
Fig. 3
Analysis of a rwCFS, and b IV-rwCFS excluding oral fluoropyrimidine anticancer drugs, with palbociclib plus ET as 1L and 2L treatment by treatment line and age group. ET endocrine therapy; IV intravenous; rwCFS real-world chemotherapy-free survival; 1L first line; 2L second line
In both the 1L and 2L treatment setting, there was a tendency towards longer IV-rwCFS in patients aged ≥ 75 years compared with younger age groups (Fig. 3b). In the 1L treatment group, median IV-rwCFS (95% CI) was 44.1 months (35.7–51.1) in patients aged < 65 years, 52.3 months (37.9–63.2) in patients aged ≥ 65 to < 75 years, and 53.2 months (40.0-NR) in patients aged ≥ 75 years (Fig. 3b). In the 2L treatment group, median IV-rwCFS (95% CI) was 30.0 months (26.6–37.1) in patients aged < 65 years, 26.4 months (22.6–35.8) in patients aged ≥ 65 to < 75 years, and 39.9 months (22.0-NR) in patients aged ≥ 75 years (Fig. 3b).
In patients receiving subsequent therapy, ET-based therapy was more common in patients aged ≥ 75 years compared with younger age groups in both the 1L (80.0%) and 2L (66.7%) setting (Table 3). In patients aged ≥ 75 years, the most common ET regimen was ET monotherapy in both the 1L (40.0%) and 2L (26.7%) settings. In contrast, CT was more common in patients aged < 65 years (1L: 36.0%; 2L: 37.3%) compared with patients aged ≥ 75 years (1L: 20.0%; 2L: 33.3%) in both the 1L and 2L setting.
Table 3 Type of subsequent therapyaIn patients receiving IV-CT as their subsequent therapy, exploratory analysis showed that median OS following IV-CT (95% CI) was 18.0 months (15.2–23.2) in patients aged < 65 years, 20.7 (15.3–23.5) in patients aged ≥ 65 to < 75 years, and NR (13.2-NR) in patients aged ≥ 75 years in the 1L treatment group (Fig. S2). In the 2L treatment group, median OS following IV-CT (95% CI) was 22.0 months (18.9–27.6) in patients aged < 65 years, 19.4 (14.3-NR) in patients aged ≥ 65 to < 75 years, and 8.9 (2.9–17.4) in patients aged ≥ 75 years (Fig. S2).
Age-stratified analyses of patients initiating palbociclib at 125 mg/dayBaseline disease characteristics and outcomes (such as rwPFS, OS and CFS) of patients initiating palbociclib 125 mg/day analyzed by age group are shown in the Supplemental Tables and Figures. Patient backgrounds, rwPFS, OS, and CFS were largely similar between the overall population and patients who initiated palbociclib treatment at 125 mg/day (Table S3–S4, Fig. S3–S4).
Comments (0)