
Remember me
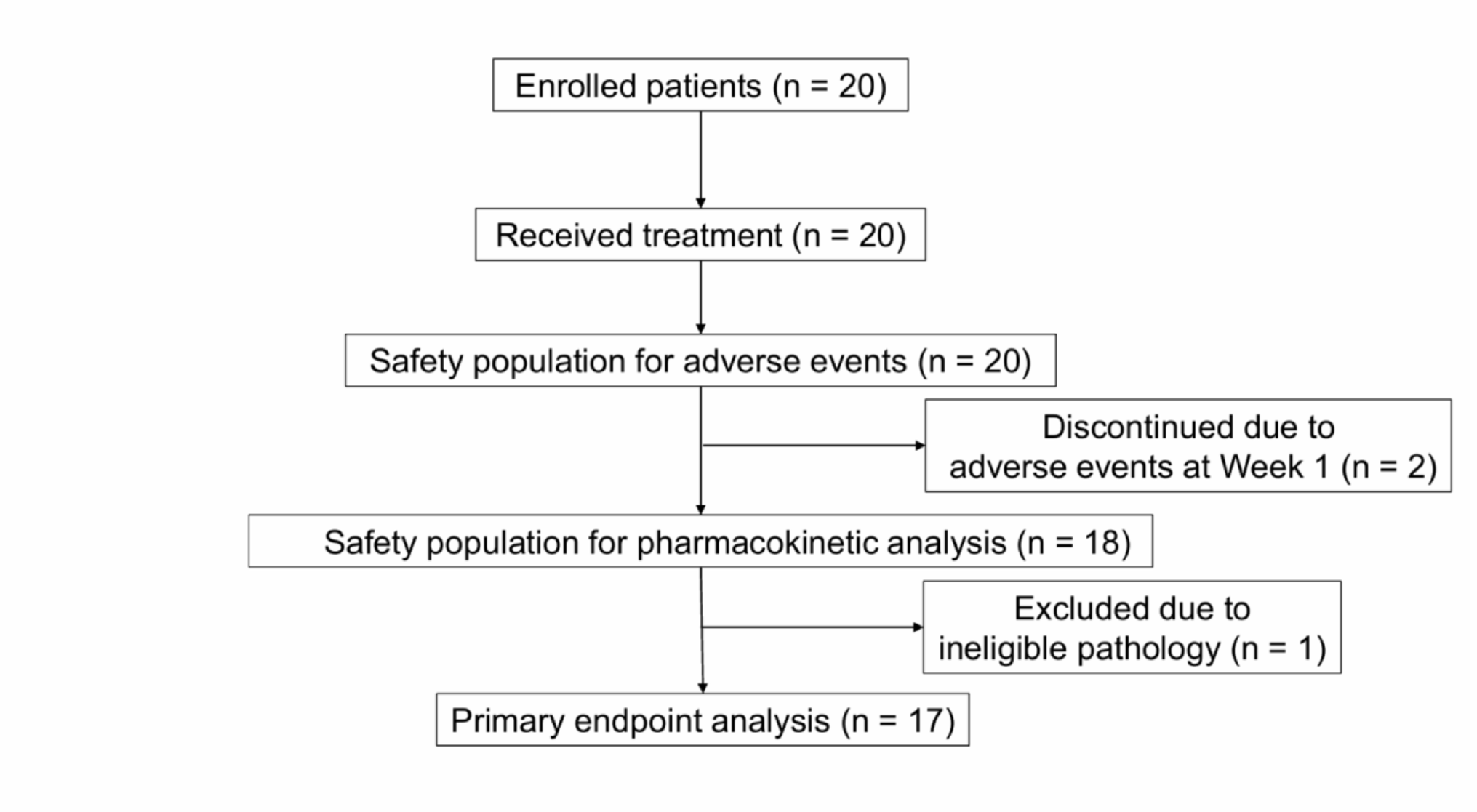
A total of 20 participants were enrolled between November 2022 and June 2024. Of these, two participants discontinued the study early during Week 1 due to Grade 1, study-related adverse events (e.g., dizziness) and were excluded from the primary analysis and pharmacokinetic evaluations. Additionally, one participant was later found ineligible based on pathological findings after treatment completion; although this participant was excluded from the primary analysis, safety data regarding adverse events were included (Fig. 1).
Fig. 1
CONSORT flow diagram of patient enrollment and analysis. A total of 20 patients were enrolled and received treatment. Two patients discontinued during Week 1 due to Grade 1 adverse events (e.g., dizziness) and were excluded from both the primary endpoint analysis and serum concentration-related safety assessments. One additional patient was later deemed ineligible and excluded from the primary endpoint analysis but included in the safety population. As a result, 17 patients were included in the primary endpoint analysis, 20 in the safety population for adverse events, and 18 in the safety population for pharmacokinetic analysis
The study population of 20 participants was subdivided as follows: Primary analysis population (n = 17), safety population for adverse events (n = 20), and safety population for pharmacokinetic analysis (n = 18). Detailed patient characteristics are presented in Table 1, while baseline characteristics are shown in Supplementary Table S1 for all participants (n = 20) and in Supplementary Table S2 for the safety population for pharmacokinetic analysis (n = 18).
Table 1 Patient characteristics for the primary analysis populationAmong the 17 eligible patients who continued treatment at Week 2, five (29.4%) underwent dose escalation to 75 mg once daily. All 17 patients completed the 4-week treatment period and 15 (88%) expressed a desire to continue venlafaxine at both study end and 3 months post-study.
Primary analysisThe weekly hot flash score, determined by a previously reported patient diary analysis protocol [12], decreased by 49.8% on average at Week 4 compared with baseline (baseline: mean 109.8, SD 74.4, median 79, interquartile range [IQR] 49 to 125; Week 4: mean 55.1, SD 56.9, median 33, IQR 11 to 75; P < 0.001). The temporal changes in hot flash scores are shown in Fig. 2. A reduction in scores was observed from the early phase of venlafaxine administration and was evident at every weekly timepoint (Week 1: mean 69.3, SD 52.7, median 54, IQR 25 to 101; P < 0.001; Week 2: mean 56.1, SD 52.9, median 44, IQR 13 to 81; P < 0.001; Week 3: mean 55.4, SD 53.9, median 37, IQR 9 to 80; P < 0.001).
Fig. 2
Weekly hot flash scores from baseline to Week 4. Box plots show weekly hot flash scores at baseline and Weeks 1 to 4. Boxes indicate the interquartile range (IQR), horizontal lines indicate the median, whiskers extend to 1.5 × IQR, and dots represent outliers. Hot flash scores significantly decreased from baseline at all time points (P < 0.001, Wilcoxon signed-rank test)
Evaluation of drug metabolism and safetyEffect of venlafaxine on TAM metabolismCompared with baseline, no significant difference was observed in serum TAM concentrations at Week 4 (baseline: mean 181.9 ng/mL, SD 57.7, median 161.0, IQR 146.0 to 212.75; Week 4: mean 164.4 ng/mL, SD 57.3, median 149.5, IQR 128.5 to 201.25; P = 0.055). Similarly, no significant reduction was observed in the serum concentrations of the active metabolites of TAM, including NDT (baseline: mean 238.1 ng/mL, SD 71.2, median 239.5, IQR 191.3 to 276.0; Week 4: mean 232.2 ng/mL, SD 78.4, median 223.5, IQR 187.0 to 285.5; P = 0.486), 4-OHT (baseline: mean 2.94 ng/mL, SD 1.34, median 2.47, IQR 2.09 to 3.17; Week 4: mean 2.84 ng/mL, SD 1.45, median 2.44, IQR 1.75 to 3.30; P = 0.442), or EDF (baseline: mean 10.25 ng/mL, SD 4.90, median 8.83, IQR 7.50 to 11.75; Week 4: mean 9.09 ng/mL, SD 5.16, median 6.48, IQR 5.76 to 12.90; P = 0.119) (Fig. 3).
Fig. 3
Serum concentrations of tamoxifen and its metabolites at baseline and Week 4. Box plots show serum concentrations of A tamoxifen, B N-desmethyltamoxifen (NDT), C 4-hydroxytamoxifen (4-OHT), and D endoxifen (EDF) at baseline and Week 4. Boxes represent the IQR, lines indicate the median, whiskers extend to 1.5×IQR, and dots indicate outliers. Paired data points are overlaid. No significant changes were observed (Wilcoxon signed-rank test, all P > 0.05)
Association between serum venlafaxine levels and CYP2D6 polymorphismsIntermediate metabolizers (IM) of CYP2D6 (n = 3) had significantly higher serum concentrations of venlafaxine at the end of treatment compared to extensive metabolizers (EM) (n = 17) (regression coefficient = 42.22, 95% CI 15.19 to 69.26; P = 0.007).
Association between serum Venlafaxine levels and hot flash scoreSerum concentrations of venlafaxine at Week 4 were not significantly associated with hot flash scores at the same time point (regression coefficient = 0.465, 95% CI − 0.524 to 1.453; P = 0.371).
Incidence of adverse eventsAll adverse events were graded as Grade 1 or 2, according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. The most frequently reported events were headache (7 patients, 35.0%), nausea (7 patients, 35.0%), insomnia (5 patients, 25.0%), dry mouth (4 patients, 20.0%), and dizziness (4 patients, 20.0%). No Grade ≥ 3 events were observed. A detailed summary is presented in Table 2 and the grade-specific and time-dependent distribution of each event is provided in Supplementary Table S3.
Table 2 Summary of adverse eventsSubgroup analysisThe reduction in hot flash scores was more pronounced with LHRH agonists (n = 12, mean reduction 56.17, median reduction 40.5, p = 0.003), In the non-LHRH group, mean and median reductions (51.0 and 70, respectively) were clinically meaningful, although these changes were not statistically significant (p = 0.063). The results are shown in Supplementary Fig. S1.
Patients without dose escalation showed a significant reduction in hot flash scores (n = 12, mean reduction 55.08, median reduction 43, p = 0.003). In the dose-escalation group, mean and median reductions (53.6 and 80, respectively) were clinically meaningful, although these changes were not statistically significant (p = 0.063). The results are shown in Supplementary Fig. S2.
Regarding CYP2D6 phenotype, a significant improvement in hot flash scores was observed in EMs while IMs exhibited a comparable downward trend that did not achieve statistical significance (Supplementary Fig. S3).
A weak negative association was observed between tamoxifen treatment duration and the percentage change in hot flash scores (Spearman’s ρ = −0.50) (Supplementary Fig. S4). The median duration of tamoxifen use before enrollment was 11.1 months (IQR, 3.0–23.5).
Venlafaxine concentrations were comparable at Week 2 (before any dose escalation; no dose-escalation group: n = 13, mean 30.2, median 20.4, p = 0.703; dose-escalation group: n = 5, mean 20.1, median 15.7, p = 0.703) while, at the end of treatment, they trended higher with dose escalation after Week 2 (no dose-escalation group: n = 13, mean 32.8, median 26.2, p = 0.117; dose-escalation group: n = 5, mean 52.6, median 55.5, p = 0.117). The results are shown in Supplementary Fig. S5.
Comments (0)