
Remember me

The following chapter presents the findings from the research study, structured according to the project’s phases and the primary outcome indicators: happiness, cognitive capacity, and physical functioning. In addition, we assess the success of each session and its potential determinants by analyzing the logbook data in relation to several contextual and participant-related factors.
The Pre-AnalysisIn the preliminary phase, data was collected through interviews, the IPLOS registry, OBS-Dementia assessments, and activity tests. In this section, we focus specifically on the interview findings to highlight residents’ perceptions of happiness prior to the intervention. The results from the other assessments will be presented and discussed in the post-analysis section, together with the corresponding post-intervention data, as changes over time are the primary focus of this study.
Interviews with the residents indicated that most participants were generally content. Of the 7 residents who participated in the interviews, three described themselves as happy, three as very happy, and one as not happy. Figure 4 illustrates the distribution of residents’ self-reported happiness levels. Several residents indicated that they occasionally feel bored and lonely, noting that their days were more enjoyable when the staff members had more time available for interaction. While one resident stated that there was little to do, others felt that there were already sufficient activities. These impressions were consistent with the responses from relatives and staff. All relatives who completed the questionnaire believed that their family member was happy or very happy, though some also reported that they residents could experience boredom in daily life. Similarly, most staff member perceived the residents as generally happy but noted that certain parts of the day – particularly mornings - could feel long and uneventful. In fact, 91% of the employees reported that they believed residents were often or very often bored. Several staff members commented that periods of inactivity, especially in the mornings, could lead residents to doze off, which in turn affect their sleep patterns. Examples of the employees’ comments include: “Due to other staff tasks, the residents may be left sitting alone in the living room for a while in the morning – then they fall asleep easily, which has a negative effect on their night’s sleep”; “They are dependent on the staff”; and “If there are no activities left to do, they sit in the living room and watch TV.”
InterventionDuring the intervention phase, a total of 266 activity sessions were documented in the activity log. Some additional sessions were conducted but not recorded, particularly early in the project when staff were still becoming familiar with the logging routines. These missing entries were non-systematic and occurred before standardized procedures were fully implemented. After the initial adjustment period, logging became consistent, and the majority of sessions throughout the remainder of the intervention were captured. Because the missing data were not associated with specific activity types or resident satisfaction levels, they are unlikely to introduce systematic bias into the analyses. The available records therefore provide a representative overview of residents’ activity patterns, levels of engagement, and satisfaction during the intervention period.
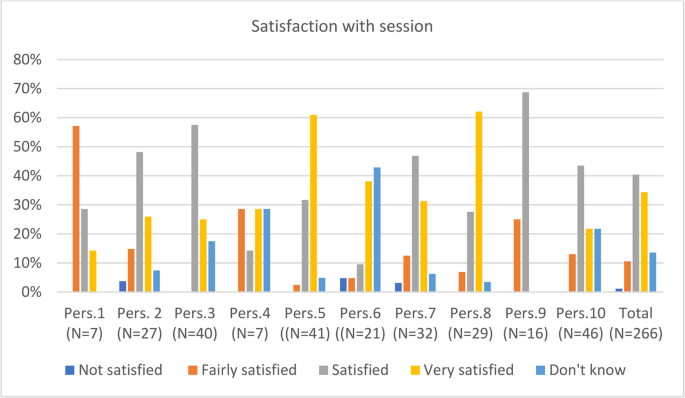
Figure 1 presents the residents’ satisfaction ratings for the Touch & Play sessions, categorized by residents. In 40% of the recorded sessions, residents were satisfied, and in 34%, the participants were very satisfied. Only 1% of the sessions were unsuccessful, where participants indicated that they were not satisfied with the session. Satisfaction level varied between individuals; while some individuals (residents 5 and 8) consistently expressed high satisfaction, other (residents 1 and 9) were less enthusiastic. Overall, the data indicate that most residents experienced a high degree of satisfaction with the sessions. The number of registered sessions per participant (N), is stated in brackets beneath each participant number. As shown, participation frequency varied considerably: for example, Participant 10 attended 46 sessions, whereas Participants 1 and 4 attended only 7 sessions each. There appears to be a tendency for participants with higher attendance (e.g., Participants 5 and 8) to report greater satisfaction compared with those who participated less frequently (e.g., Participants 1, 7, and 9). However, it is difficult to state whether there is a causal relationship, as the causal relationship could just as well apply in the other direction.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.The various participants’ satisfaction with the sessions
To examine whether session success was influenced by the session duration, time of day, type of activity or number of participants, we analysed variation in satisfaction across these parameters. Figure 2a displays satisfaction ratings stratified by session length. The length of the session varied between 2 and 180 min, but most (88%) were between 30 and 60 min. As shown in the figure, sessions of medium duration (31–45 min) yielded the highest satisfaction scores. For shorter sessions, the causal connection is unclear – it is possible that the shorter sessions were terminated early due to residents’ apparent dissatisfaction and limited engagement. To further assess the relationship between duration and satisfaction, a Spearman correlation analysis was conducted; this test revealed no significant association between the two variables, indicating that session length alone was not systematically related to residents’ satisfaction levels.
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a:Satisfaction with session by length of session; b: Satisfaction with session by time of day; c: Satisfaction with session by number of participants; d: Satisfaction with session by activity level
Figure 2b illustrates the association between time of day and session satisfaction. Morning sessions were the most successful, and they also represented the majority of conducted sessions. Specifically, 67% of all registered sessions took place in the morning (10:00–12:00), 27% in the afternoon (12:00–18:00), and only 5% in the evening (after 18:00).
Figure 2c illustrates the relationship between group size and session satisfaction. Participation per session varied, although nearly half (47%) of all sessions involved only one resident together with a staff member. As group size increased, the proportion of sessions in which participants were very satisfied and satisfied decreased, while the proportion of sessions rated as only fairly satisfied and not satisfied increased.
Type of activity also influenced the success of each session. A review of the logbook comments and post-intervention staff interviews shows that activities involving music and reminiscence—such as listening to familiar songs, singing together, watching well-known television programs, and viewing historical photographs—were regarded as particularly effective in engaging residents. Competitive games, including those in which residents throw objects to hit a target on the screen, were also frequently highlighted as enjoyable and motivating. As one staff member observed, “The residents are still competitive, and competitions for the highest score are popular.” In contrast, activities that were cognitively or physically demanding, such as “catching mice” or “swatting flies” on the screen, were perceived as less successful. Staff explained that tasks exceeding residents’ abilities may reduce motivation, stating, “What they don’t master becomes boring.” A substantial proportion of sessions (41%) included elements of physical engagement. As illustrated in Fig. 2d, sessions involving physical activity were generally associated with higher satisfaction levels, although some variability in participants’ responses persisted.
To examine whether session success varied according to dementia severity, we linked data from the OBS-Dementia assessments with the logbook records. Figure 3 presents the shares of sessions rated as very satisfied, satisfied, or fairly satisfied across different levels of cognitive impairment. Dementia severity was assessed using the OBS-Dementia scale, where lower scores indicate more advanced dementia and higher scores reflect less severe impairment. Substantial variability was observed, and no definitive pattern emerged. However, the trend lines indicate a slight negative slope for sessions rated as very satisfying and a positive slope for sessions rated as satisfying or fairly satisfying. This suggests a tendency for residents with less severe dementia to more frequently report sessions as satisfying or fairly satisfying, whereas residents with more advanced dementia more often reported being very satisfied with the sessions. (Figure 3.)
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Satisfaction with session by degree of dementia (OBS dementia score)
Post-AnalysisThe post-analysis is essential for evaluating the impact of Touch & Play. By comparing the post-intervention results with the pre-intervention findings, we can estimate the extent to which the technology has influenced the key outcome measures related to happiness, cognitive capacity, and physical functioning.
HappinessAfter one year of implementing Touch & Play, follow-up interviews were conducted with residents, relatives, and staff to capture updated perceptions of happiness. The resident interviews showed that all participants reported feeling fairly happy, happy, or very happy in their daily life at the nursing home. Notably, no residents indicated being not happy. One resident who had previously reported being not happy prior to the intervention now described feeling fairly happy, and another reported an improvement from happy to very happy. For one resident, however, the reported level of happiness declined slightly from very happy to happy. The remaining residents reported the same level of happiness as before. Figure 4 illustrates the distribution of residents’ self-reported happiness levels at baseline and after one year of Touch & Play use.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Residents’ self-reported happiness before and after one year of using touch & play.
All residents reported that they enjoyed engaging with the activity board. Several further noted that Touch & Play allowed them to take a more active role in selecting activities and entertainment opportunities that had not been mentioned prior to the intervention. Although residents had not previously expressed a need for greater influence over activity planning, they now appeared to appreciate this enhanced sense of involvement and co-determination.
The residents’ reported level of happiness was corroborated by responses from both relatives and staff. Several relatives believed that Touch & Play had contributed to increased happiness for their family member, and all staff participants reported similar impressions. Staff emphasized that the technology fostered positive engagement, noting for example that residents “recognize the screen, and … associate it with something positive”, that it “encourages engagement in singing, and stimulates talking and laughter”, and that “increased physical activity creates a better social environment.” At the same time, staff also highlighted the importance of considering the nature of advanced dementia. One employee remarked that “the screen often appears to enhance residents’ happiness; however, many residents occasionally do not recognize the device or report that they have never seen or used it before…”.
Overall, staff expressed strong support for the implementation of the Touch & Play project and generally reported that its introduction had not replaced or reduced other existing activities. Most employees indicated that the use of Touch & Play had little or no impact on their workload. One staff member felt that it had resulted in a slight increase in work, whereas another reported a reduction in workload due to decreased restlessness and challenging behaviors among residents. The latter view aligns with findings presented in the subsequent section.
Physical and Cognitive CapacityTo assess whether Touch & Play had an effect on physical functioning and cognitive capacity, standardized tests were administered both prior to implementation and again after one year of use. When interpreting these findings, it is important to acknowledge that participants were individuals with advanced dementia, for whom progressive decline in these abilities is anticipated. The purpose of the comparison was therefore not necessarily to identify improvements, but rather to determine whether the rate of decline over time appeared reduced or less pronounced than expected. In this way, the analyses sought to explore whether the intervention may have had a stabilizing or moderating effect on cognitive and physical deterioration.
Table 2 presents the average OBS-Dementia scores across the different categories and subcategories. The total score provides insight into the overall functional status, whereas the subcategory scores offer a more detailed indication of developments within specific domains. In addition to showing the change in scores over the one-year intervention period, the table reports the participants’ average pre-intervention and post-intervention scores. The OBS-Dementia scale ranges from 0 to 6, where a score of 6 indicates intact functioning and a score of 0 indicates no functioning. Accordingly, a negative change in score reflects a decline in the functional level for the respective category.
Table 2 Average change in the OBS dementia score, divided into different categories and subcategoriesOverall, the mean OBS-Dementia score declined by 0.594 points across all participants and categories over the one-year period. However, substantial variation was observed between individuals and across categories. Among the different participants smallest overall reduction was 0.19 points, whereas the largest was 0.97 points, indicating differing rates of functional decline among participants.
To investigate whether the frequency of Touch & Play use influenced changes in cognitive functioning, we analyzed the relationship between the number of logged sessions and the change in OBS-Dementia scores (Fig. 5). The results were not definitive; however, a weak negative correlation was observed, indicating that more frequent engagement with Touch & Play may be associated with a slower decline in cognitive functioning. These findings must be interpreted with caution, and further studies with larger samples are required before any conclusions can be drawn about potential protective effects.
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.The relationship between change in OBS dementia score and use of Touch & Play
Substantial variation was also observed across the categories assessed. As shown in Table 2, memory, orientation, and self-care abilities demonstrated the greatest decline over the study period, whereas emotional functioning showed only a modest reduction. Notably, social functioning has improved overall. Staff attributed this improvement to increased participation in shared activities, greater initiative among residents to socialize, and strengthened relationships between residents following the introduction of Touch & Play.
Within the emotional functioning category, the relatively minor decline appeared to be related to reductions in restlessness and disruptive behavior, alongside a pronounced decrease in anxiety levels. These findings align with previous research from Denmark, which reported that comparable technology could contribute to calming and redirecting individuals with dementia who experience agitation or wandering behaviors (Langvald, 2015). Moreover, the score in the subcategory mood remained stable, in contrast to the gradual deterioration observed in most other categories. An equal number of residents experienced positive and negative changes in this subcategory. These results reinforce the interview and survey findings, indicating that overall happiness remained high and may have been positively influenced by the Touch & Play intervention.
The IPLOS assessment measures several of the same domains as the OBS-Dementia test, but with a different emphasis. As such, the IPLOS results serve as a valuable complement to the OBS-Dementia findings and provide additional insight into residents’ cognitive and functional development. It is important to note that the IPLOS scale ranges from 1 to 5, where a score of 1 indicates the highest level of functioning and 5 the lowest, representing the opposite direction of the OBS-Dementia scale.
Table 3 reports the overall average change IPLOS score broken down by the change in the various categories. The average increase in the total IPLOS score was found to be 0.525, but there was great variation among the participants. Participants with the highest increase had an increase of 1.2, but there were three participants who had no change in their score over the test period.
Table 3 Average change in IPLOS score by different categoriesIn Table 3, the average changes in scores across the different categories are presented in ascending order of magnitude. The category showing the least change was managing personal finances, with an average change of 0.00 points. This lack of change is explained by the fact that all participants already demonstrated no functional ability in this area prior to the intervention and continued to score at the same level afterward.
The second smallest change was observed in the memory category, with an average increase of only 0.13 points. All but one participant maintained a stable memory score throughout the intervention period. This finding is noteworthy, as one of the project’s initial hypotheses was that Touch & Play might help to sustain or strengthen cognitive functioning. Similarly, social participation showed relatively limited change. Four of the eight participants demonstrated stable scores, and one participant showed a slight improvement (i.e., a lower score), suggesting enhanced social functioning. These results are consistent with the qualitative findings presented earlier, indicating that Touch & Play may have supported social cohesion and social functioning among residents.
Additionally, indoor and outdoor movement exhibited minimal deterioration over time. With the exception of one participant who was immobilized due to injury, all residents maintained stable mobility scores, which may indicate a positive influence of the intervention on physical functioning.
The physical assessments also provide insight into changes in physical functioning. These tests measured walking speed, grip strength, and the time required to stand up and sit down, and they were administered by the nursing home staff. For most participants, performance declined across all measures over the intervention period, which aligns with expectations for individuals with advanced dementia. However, there were notable exceptions: two participants demonstrated improved grip strength after one year. Interestingly, one of these individuals was among the most active users of Touch & Play and had the highest number of registered sessions in the logbook.
Weaknesses of the ProjectThe primary limitation of this project is its small scale. Only ten residents were followed over the one-year period, which restricts the statistical power of the analyses and limits the ability to draw firm conclusions regarding the effects of Touch & Play. A larger sample size would have strengthened the robustness and generalizability of the findings.
Furthermore, the implementation of Touch & Play was not fully standardized. A more structured intervention protocol—with fixed session frequency, duration, and activity types—could have enabled a clearer assessment of dose–response relationships and intervention fidelity.
Another important limitation is the absence of a control or comparison group. Without a reference group that did not receive the intervention, it is difficult to attribute observed changes exclusively to Touch & Play, as opposed to the natural progression of dementia or other contextual factors.
A further limitation relates to incomplete logging of activity sessions, particularly during the early stages of the project before standardized recording routines were established. Although the missing entries appear to have been non-systematic, their absence reduces the completeness of the dataset and may limit the precision of some descriptive analyses. All statistical and descriptive assessments were therefore based solely on the available logged sessions, and results should be interpreted with this constraint in mind.
Comments (0)