Within this conceptual framework, our findings may also be interpreted in light of the emerging paradigm of antimicrobial heteroresistance. In our study, we detected a remarkably high prevalence of CHR (61.4%) among COL-susceptible P. aeruginosa bloodstream isolates using the PAP method, considerably higher than the results of previous studies conducted. Notably, the GT failed to identify any heteroresistant strains, highlighting the limitations of conventional susceptibility testing methods in detecting minority resistant subpopulations. Furthermore, since there are limited studies investigating the effect of HR on clinical outcomes, in the present study, we found that age ≥ 60, lack of hospitalization history, and a colistin MIC of 1 mg/L were risk factors for CHR. However, no significant association was observed between CHR and mortality.
The remarkably high prevalence of CHR observed in our study warrants careful interpretation. Several methodological and epidemiological factors may have contributed to this finding, including differences in heteroresistance definitions and PAP interpretation criteria. Previous studies have applied different resistant-subpopulation frequency thresholds (e.g., 10⁻⁶ versus 10⁻⁷), different concentration cut-offs, and different PAP interpretation approaches. Consequently, direct comparison of CHR prevalence across studies should be made with caution, and the prevalence observed in our study may not be directly comparable to previously published reports. Although the prevalence observed in our study was higher than most previously reported rates, relatively high CHR frequencies have also been reported in studies using PAP-based methodologies [10]. This observation may suggest that at least part of the variability across studies reflects true epidemiological differences in addition to methodological heterogeneity. Nevertheless, the lack of an internationally standardized definition of colistin heteroresistance remains a major challenge for cross-study comparisons and highlights the need for consensus criteria for CHR detection. The available literature on colistin heteroresistance in P. aeruginosa is summarized in Table 4.
Table 4 Summaries of studies on colistin heteroresistance in P. aeruginosa isolatesIn addition to methodological variability, epidemiological characteristics of the study population and local antimicrobial selection pressures may also have influenced the observed CHR prevalence. Only 21% of patients had documented prior colistin exposure, suggesting that previous colistin therapy alone cannot explain the high prevalence of CHR observed in our study. The high prevalence of CHR may be influenced by factors beyond individual antibiotic exposure. Clinically achievable plasma colistin concentrations are limited by toxicity concerns and may not completely suppress resistant-subpopulations, potentially facilitating their persistence [5]. Furthermore, sustained colistin use in our hospital setting may have contributed to the maintenance and circulation of heteroresistant strains within the healthcare environment. These factors may partly explain the high frequency of CHR detected among bloodstream isolates in our study. Additionally, CHR has been reported more frequently among multidrug-resistant and carbapenem-resistant strains. Since our collection largely consisted of isolates recovered from a tertiary-care hospital with a high burden of resistant Gram-negative bacteria, the high CHR rate observed in our study may be associated with the predominance of resistant hospital lineages rather than prior colistin exposure alone [16]. The markedly lower CHR prevalence reported in the recent Iranian study may further illustrate the substantial variability observed across studies [15]. In addition to differences in PAP interpretation criteria, the two studies differed considerably in isolate selection. While the Iranian study included clinical isolates from various infection sites, our study was restricted to bloodstream isolates and predominantly included strains with colistin MICs of 1–2 mg/L, a factor independently associated with CHR in our cohort. Therefore, differences in study populations and isolate characteristics may have contributed to the discrepant prevalence estimates.
Another possible explanation for the high prevalence observed in our study is the composition of the isolate collection. Only bloodstream isolates with colistin MICs of 1–2 mg/L were included, and isolates with a MIC of 1 mg/L constituted the majority of the study population. Notably, a colistin MIC of 1 mg/L was independently associated with CHR, suggesting that the MIC distribution within the study sample may have contributed to the observed prevalance estimate. Since isolates with a MIC of 1 mg/L were independently associated with CHR in our cohort, the distribution of MIC values within the study population may have contributed to the observed prevalence estimate. This finding is noteworthy because it challenges the conventional assumption that higher MIC values necessarily indicate a greater likelihood of resistance-related phenomena. Instead, it suggests that isolates categorized as fully susceptible may still contain resistant subpopulations detectable by PAP. While the proportion of isolates with a colistin MIC of 1 mg/L in the study by Howard-Anderson et al. (66%, n = 95) was similar to that observed in our cohort, those authors did not identify a significant association between MIC category and CHR, in contrast to our findings [14].
The biological basis of stable and unstable heteroresistance remains incompletely understood. Stable heteroresistance may suggest the presence of heritable alterations that allow resistant subpopulations to maintain their phenotype after serial passages in antibiotic-free media. In contrast, unstable heteroresistance may reflect reversible adaptive responses to antibiotic exposure, including transient phenotypic switching or persistence-like states [6, 7]. Such mechanisms could permit survival during antibiotic treatment while not being permanently maintained in the bacterial population. Because the present study did not investigate the molecular mechanisms underlying heteroresistance stability, these interpretations should be considered speculative and require confirmation by future genomic and transcriptomic studies.
In the current study, the clinical response rate was statistically higher in the CHR-positive group than in the CHR-negative group (p = 0.042). It is crucial to highlight that the number of patients receiving colistin-based regimens in our cohort was highly limited (n = 13); therefore, this difference in clinical outcomes cannot be attributed to the choices or efficacy of colistin therapy. Importantly, this counterintuitive finding was not driven by baseline clinical disparities between the two groups. Major clinical determinants and confounding factors that directly influence prognosis—including the CCI, severe immunocompromised status, presence of sepsis at onset, meropenem resistance rates, the administration of in vitro active antibiotics, and colistin-based therapy—were highly comparable and showed no statistically significant differences between the CHR-positive and CHR-negative groups (Table 2). Given that these key clinical variables were well-balanced between the groups, the biological basis of the higher clinical response rate observed among CHR-positive patients remains unclear. One possible explanation may be the fitness cost associated with heteroresistance. However, this hypothesis was not directly evaluated in the present study and requires confirmation in future experimental investigations. Additionally, consistent with the findings of a previous study [14], no significant association was observed between CHR and overall mortality in our cohort. As with the clinical response rates, this lack of association cannot be attributed directly to the definitive clinical effect, or lack thereof, of the CHR phenotype, due to the small size of the subpopulation treated with colistin. Therefore, future prospective studies with larger cohorts of colistin-treated patients, complemented by molecular and genomic analyses, are warranted to fully elucidate the definitive clinical trajectory and underlying genetic mechanisms of colistin heteroresistance in bloodstream infections.
Another notable finding was the association between the absence of recent hospitalization and the presence of CHR. While hospitalization is traditionally considered a risk factor for antimicrobial resistance, this observation may indicate that heteroresistance is not solely driven by nosocomial selective pressures. This observation should be interpreted cautiously and validated in future studies. Furthermore, increasing age, which emerged as another independent predictor of CHR in our multivariable model, is a well-known risk factor for resistant P. aeruginosa infections [17].
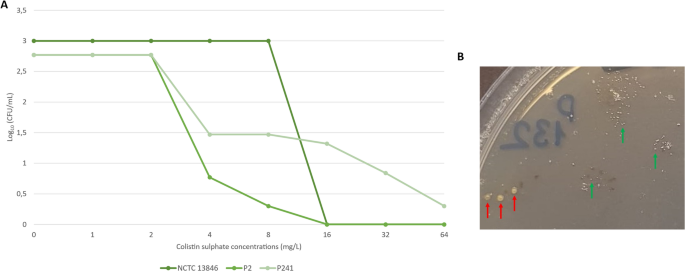
Even though the PAP method is regarded as the most reliable method for detecting HR, its high cost and labor-intensive nature make it difficult implement in clinical settings. Therefore, diffusion-based tests are widely utilized in clinical microbiology laboratories, particularly in countries with a high prevalence of HR. In the present study, no bacterial growth was observed within the inhibition zone of colistin GT strips for any of the isolates identified as heteroresistant by the PAP method. Standard susceptibility testing methods may overlook clinically significant minority variants, potentially leading to underestimation of resistance and suboptimal treatment decisions. This limitation underscores the need for diagnostic approaches capable of capturing population-level complexity. This suggests that GT testing is insufficient for detecting CHR, a finding consistent with previous studies [18, 19]. The limited diffusibility of colistin on agar surfaces may account for the failure to detect CHR, similar with the limitations of diffusion-based techniques in determining colistin susceptibility.
The observation of distinct colony morphologies within heteroresistant subpopulations in one isolate further supports the concept of phenotypic diversification within bacterial populations. Although heteroresistance and small colony variant phenotypes are considered as distinct, our findings suggest that these two phenotypes may not be entirely separate concepts and could potentially overlap [20]. To our knowledge, no study in the literature presents data similar with our observation.
Our study has several limitations. First, it was conducted retrospectively and included a relatively small number of isolates. The small sample size in our multivariable analysis resulted in wide confidence intervals for certain predictors; therefore, these identified risk factors for CHR should be interpreted with caution and validated in larger cohorts. Second, our analysis was based on culture-dependent methods and did not incorporate molecular or metagenomic approaches that could better characterize microbial population diversity. Therefore, the underlying mechanisms driving heteroresistance and its relationship with the broader bloodstream microbial environment remain to be elucidated. Third, PAP experiments were performed once for each isolate and formal reproducibility or inter-run variability analyses were not performed. Finally, the classification of stable and unstable heteroresistance was based on a seven-day serial passage protocol and should be interpreted in the absence of a standardized definition for heteroresistance stability.




Comments (0)