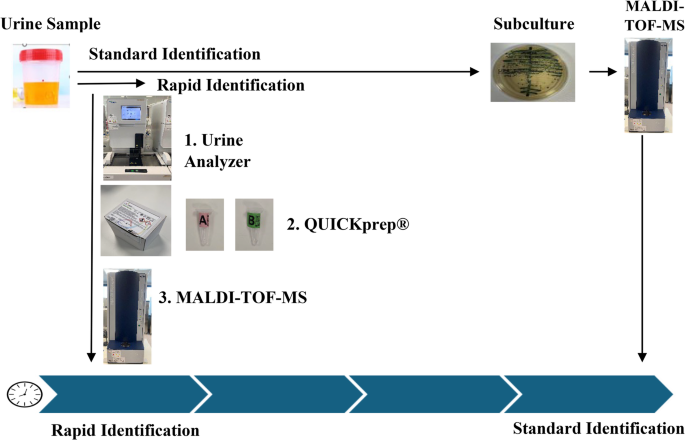
Direct, rapid, and accurate ID of microorganisms from clinical samples—bypassing culture and shortening turnaround time by 1 day—supports timely clinical decision-making. The therapeutic approach may vary significantly depending on whether the pathogen is a cocci, a bacilli, or a yeast, and between different bacterial species, such as, for instance, Escherichia coli or Pseudomonas aeruginosa, even representing only a small percentage. Although rapid identification cannot replace AST, it provides valuable guidance for empiric therapy and facilitates the prompt initiation of a standard AST, as the selection of antibiotics depends on that, or even the decision not to proceed due to contamination. Regarding rapid AST, such as the FASTinov assays, it demands a rapid ID not only to select the adequate antibiotics (FASTgramneg or FASTgrampos) but also for the interpretation of breakpoints, being in certain cases species-specific, impacting on report.
This approach directed at urine samples was only feasible due to the availability of advanced urine screening methods, such as Sysmex analysers which, not only identify negative samples, avoiding culture, but also provide valuable information in positive cases. These include bacterial load (number of bacteria per urine volume), infection-related parameters (e.g., leukocytes and red blood cells), potential contamination, and even an indication of the Gram status of the microorganism—Gram-positive, Gram-negative or yeasts.
The kit QUICKPrep® from FASTinov® is a rapid and reliable method for identifying both Gram-negative, Gram-positive bacteria and yeasts. Inoculated samples were used to increase the variability of microorganisms and 100% of correct identifications were obtained as they were pure cultures. In clinical samples, 11% could not be identified, likely due to sample contamination. While the use of formic acid can improve identification in some organisms, it does not solve issues related to mixed microbial populations. In five clinical samples, more than one microorganism was identified—an important finding, as no AST method could be performed in polymicrobial samples. Overall, in 18 out of 115 clinical samples (~ 16%), 13 had no identification and 5 had multiple species detected, all likely due to contamination. When no ID or mixed population is obtained, we should not proceed with AST, or incorrect results would be obtained. This underscores a key limitation of direct-from-sample testing: the absence of a pure culture can compromise downstream analyses. This brings up the topic of the importance of sample collection.
When compared to the other protocols for direct ID from urine [8,9,10], the QUICKprep kit provides a very “clean” pellet due to its protocol responsible for the high scores obtained on MALDI-TOF-MS. This is also an advantage for any AST methods. The accuracy of determining the concentration of microorganisms is very high. This procedure enables the accurate use of the McFarland scale to perform the quick FASTinov AST method based on flow cytometry directly from positive blood cultures [13] or any other method.
Despite the transformative impact of MALDI-TOF-MS technology in microbiology, it still presents some limitations namely, the requirement for a high bacterial load and the need for a clean, interference-free sample. The FASTinov® QUICKprep® was specifically developed to concentrate and purify biological specimens, enabling accurate MALDI-TOF-MS identification while preserving microbial viability. This preserved viability allows subsequent diagnostic applications, such as phenotypic AST and represents a significant advantage in terms of both time and resource efficiency.
In conclusion, the QUICKprep® kit represents a reliable method for the direct ID of microorganisms in urine samples, however, a higher number of clinical samples are needed to be tested. Nonetheless the ones presented in our study are the more frequently found in the clinical routine.




Comments (0)