
Remember me
This post hoc study of the ROSE randomized trial assessed adherence and determinants for adherence among ROSE participants and the general population, utilizing survival analyses of clinical data from the ROSE study and data from nationwide registers.
The ROSE study and data sourcesDetails of the ROSE study have been published [7, 8]. In brief, 98,383 women aged 65–80 residing in the Region of Southern Denmark in 2010 were identified. A random sample of 34,229 women was selected for participation in the ROSE study and randomized to either a screening or control group. All participants (both from the screening group and controls) received an invitation letter by mail in 2010–2011 that contained a questionnaire comprising questions on clinical risk factors for calculating FRAX. Only women in the ROSE screening group with moderate to high fracture risk assessment, assessed as a major osteoporotic FRAX score of ≥ 15%, were offered the intervention, which included a DXA scan of bone mineral density of the lumbar spine (L1–L4) and total right hip. A diagnosis of osteoporosis was based on the lower of the two BMD values. If osteoporosis was identified by bone mineral density (BMD) T-score < − 2.5 SD, treatment advice according to the Danish guidelines [10] was provided to both the women and their GPs, with the GP responsible for the treatment.
The Danish Civil Registration System Register [17] provided baseline demographic data, migration, and vital status. Socioeconomic data came from Statistics Denmark [18]. Prescription data, derived from the Danish National Prescription Registry [19], included data on all filled prescriptions at Danish pharmacies from 1995 and onwards, coded using the Anatomical Therapeutic Chemical Classification System (ATC) and Defined Daily Dose (DDD). Hospital diagnoses (coded according to the International Classification of Diseases, 10th Revision (ICD-10)) and codes for treatment administered during hospital contacts were obtained from the Danish National Patient Register [20], which keeps records of all inpatient and outpatient hospital contacts since 1995. The personal identification numbers were used to link data on an individual level.
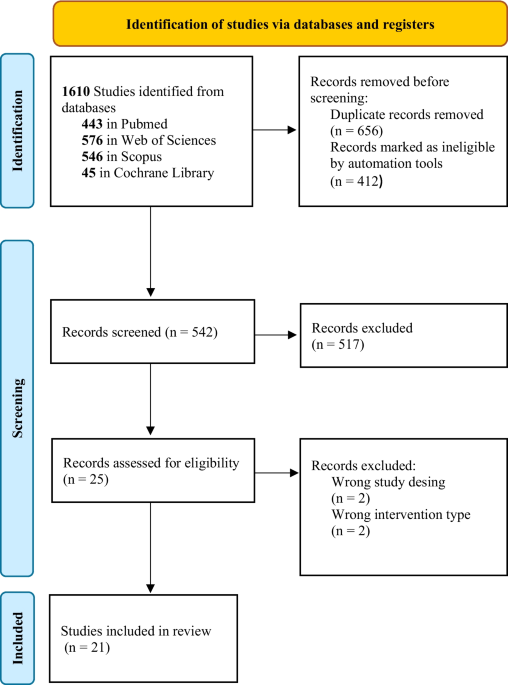
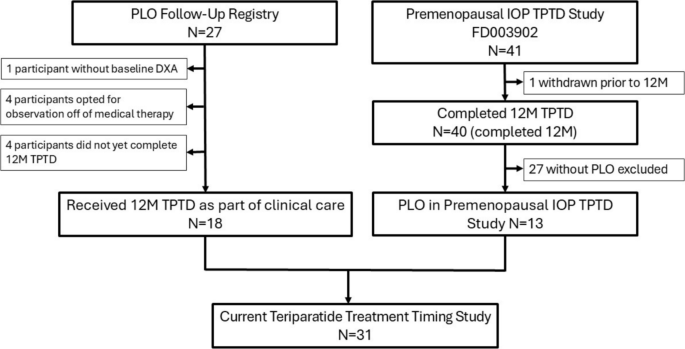
Study populationFigure 1 depicts the flowchart of the study population. A total of 17,072 women were randomized to the ROSE screening group (group A) and 17,157 to the ROSE control group (group B). We defined the study-baseline as the date the ROSE participants returned the ROSE questionnaire. We excluded ROSE participants with missing/inadequate data from the questionnaires (n = 6661/6663) and participants with self-reported AOM treatment or a record of AOM treatment within 1 year before baseline (n = 1224/1279). We also excluded participants with a primary or secondary hospital diagnosis of cancer (ICD10: C00-C99, D00-D48) or Paget’s disease (ICD10:M88) within the 5 years preceding the baseline (n = 1312/1378) and participants with missing data on sociodemographic factors (n = 103/104). These exclusions left 7772 from the screening group (A) and 7733 from the control group (B). We further restricted the population to ROSE participants with FRAX ≥ 15% (i.e. women eligible for the intervention, a DXA scan). This resulted in 5864 women from the screening group (A) and 5790 from the control group (B) constituting the study population.
Fig. 1
Flowchart for the (A) ROSE screening group, (B) ROSE control group, and (C) general population. AOM, anti-osteoporotic medication, DXA, dual-energy x-ray absorptiometry
Participants in the ROSE study represent a selected sample that may not fully reflect the general population [21]. Additionally, responses to the osteoporosis risk survey could potentially have influenced the behaviour of the ROSE participants. To address these limitations, we included a comparison group of age-matched women (group C) from the general population, who were not exposed to the ROSE survey. This comparison group provided a more natural benchmark for assessing adherence, had the screening programme been implemented more broadly, than the ROSE control group. Using the Danish Civil Registration System Register, which keeps information on all residents in Denmark, we extracted this secondary comparator group (C) from the 64,154 women residing in the Region of Southern Denmark in 2010 who were not invited to participate in the ROSE study. These women were age-matched with the ROSE participants (ratio 1:1) and sampled with replacement, allowing the possibility of selecting the same woman more than once. No other matching factors were applied than age, in order to maintain the group’s comparability with the general population. Before matching, exclusions concerning AOM treatment, diagnoses of cancer and Paget’s disease, and missing sociodemographic data were executed for the age-matched general population (C). The age-matched women from the general population (C) were assigned the same baseline date as their matched ROSE participants (A and B). Similar to the ROSE control group (B), the age-matched women (C) underwent DXA scanning and received treatment based on the standard case-finding approach used in Denmark.
Clinical covariates and determinants obtained from the ROSE questionnaireClinical data on ROSE participants was obtained from the baseline questionnaire. We assessed the following clinical determinants for adherence to treatment: previous fractures, parental history of hip fracture, current smoking status, rheumatoid arthritis, condition related to secondary osteoporosis as defined by the FRAX list, body mass index, early menopause, increased fall-risk assessed as > one fall within 12 months, and long-term immobilization. In the ROSE screening group, indication for AOM treatment based on the DXA finding was also evaluated as a determinant for adherence.
Covariates and determinants derived from the national registersWe obtained data on baseline characteristics from the Danish national registers for the entire study population (group A, B, and C), which included age, cohabitation status, disposable family income, and highest obtained educational level in the household. We also obtained information on number of redeemed co-medications (utilizing the first three ATC characters), redeemed systemically acting glucocorticoids (at least one redemption of medicine with ATC code: H02AB01-2, H02AB04-9, H02AB10, H02AB13 disregard dose and duration), and redeemed psychotropic medication (at least one redemption of medicine with ATC code: N05A-C*, N06* disregard dose and duration) in the year preceding baseline. We calculated the Charlson comorbidity index (CCI) [22, 23] based on ICD-10 hospital diagnoses recorded within the 15 years preceding the baseline.
Outcome measures: anti-osteoporosis medications (AOM)We used a composite measure for AOM treatment that included both treatment with tablets and injections. Information on redeemed prescriptions of AOM was derived from the Danish National Prescription Registry [19] and information on AOM treatment provided during hospital contacts was obtained through the Danish National Patient Register [20]. ATC codes included G03XC01 (SERM), M05BA01, M05BA04, M05BA06, M05BA07, M05BB03 (bisphosphonate), M05BX03, M05BX04 (other antiresorptives/mixed), and H05AA02 (parathyroid hormones analogues). Procedure codes included BWHB40B (ibandronate), BWHB42 (denosumab), and BWHB40A (zoledronate). See Table SI1 for more information on applied codes. We also utilized the date of filled prescription/procedure and the DDDs [24].
We evaluated long-term adherence employing the taxonomy suggested by Vrijens et al. [25]. Initiation of treatment was assessed as the date the women claimed their first AOM prescription or had their first hospital-record of AOM treatment during the observational period (until December 31, 2021) and handled as a time-to-event variable. Implementation of the dosing regimen refers to the extent to which a patient’s actual dosing corresponds to the prescribed daily dose [26]. Implementation was operationalized as the Medication Possession Ratio (MPR) = total days’ supply of medication / number of days in the observation period [27]. We considered MPR of < 80% as insufficient treatment implementation (yes/no). The MPR was calculated at each recorded treatment based on the cumulative days’ supply and the total days in the period up to that point. The first occurrence of MPR < 80% was evaluated as a time-to-event variable. Persistence with treatment is the time from initiation of treatment until discontinuation, calculated as the number of days a patient was in possession of a medication to the first gap in the therapy of greater than 90 days. We assessed the date of treatment discontinuation as a time-to-event variable.
During hospital admissions, routine treatments is generally continued, but not all treatments administered during hospitalization are recorded in the registers. We considered women as adherent during admissions. When evaluating the overall treatment of AOM, we deemed women who switched from one drug to another as adherent as long MPR was retained above 80% or persistent until the first refill gap exceeded 90 days. We did not assess adherence during medication re-initiation after MPR < 80% or discontinuation.
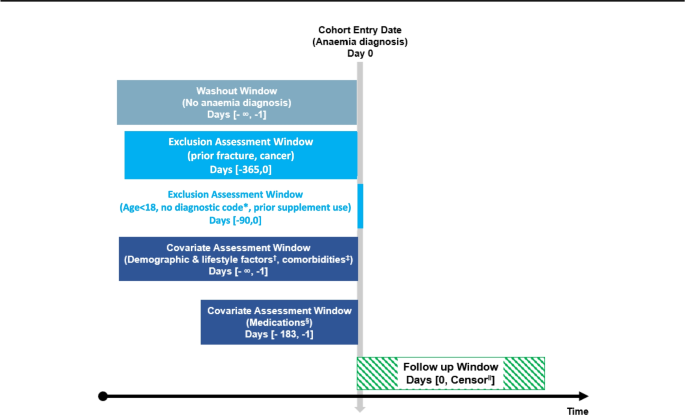
Entry date and follow-upWhen studying initiation of AOM treatment, we assessed time to first record of AOM treatment. Women in the ROSE screening group who were eligible for a DXA scan (i.e. had a FRAX ≥ 15%) had their scan a median of 195 days after the baseline date. To accommodate this left truncation, scanned women entered the risk set at the scan date. For the remaining women, we imputed an entry date using the median days above. Supplementary Fig. SI1 shows the study diagram.
The analyses assessing the implementation (MPR) of the dosing regimen and treatment persistence/discontinuation were restricted to women who initiated AOM treatment within 1 year after they were DXA scanned or an imputed date (defined as the entry date above). For these analyses, the women entered the analyses when they claimed their first AOM prescription or had their first hospital-record of AOM treatment. Supplementary Fig. SI2 shows the study diagram.
In time-to-event analyses, the study population was followed until outcome occurred or the first censoring event: diagnosis of cancer or Paget’s disease, death, emigration, or December 31, 2021.
Statistical analysisWhen assessing baseline characteristics, frequencies and percentages were used to present binary and categorical variables, while medians with interquartile range (IQR) were used to summarize continuous variables. We calculated the cumulative incidence function (CIF) of initiation of AOM treatment using the Aalen-Johansen estimator [28]. The survival probability of high treatment implementation (MPR ≥ 80%) and persistence over time was computed using the Kaplan–Meier method. We studied the relative differences in adherence between the ROSE screening group (A), the ROSE control group (B), and the age-matched general population (C) using Cox regression models adjusted for age at baseline (included as cubic splines) and CCI (0, 1, ≥ 2). We tested the proportional hazard assumption utilizing log–log plots and by plotting Kaplan–Meier versus predicted survival. To accommodate that the assumption was not met for the Cox model assessing initiation, the analysis-time was split at 1 year, 3 years, and 5 years. We also used multivariate Cox regression models to examine the association of determinants for initiation of treatment within the first year of follow-up and determinants for discontinuation (non-persistence) within the first year and second-tenth year after initiation of treatment. The models were adjusted for potential confounding variables specific to each determinant. Estimates for the Cox regression models are presented as hazard ratios (HRs) with 95% confidence intervals (95% CI). The analyses were performed in StataMP18.
Registration and ethicsThe ROSE trial is registered at ClinicalTrials.gov (NCT01388244) and approved by the Regional Committee on Health Research Ethics for Southern Denmark (jr.nr S-20090127) and the Danish Data Protection Agency. The analyses in this publication are post hoc analyses.
Comments (0)