
Remember me
Baseline characteristics of women with or without any VF, according to the method used (manual VFA or XVFA), are presented in Table 1. In total, 423 women were included in the analysis. When VFAs were annotated manually or by XVFA, 102 (24%) and 187 (44%) women, respectively, were identified as having any VF. In both methods- manual and XVFA- women with any VF were older, had lower BMD by DXA, and higher FRAX 10-year probabilities for MOF and hip fracture compared with women without VF (p < 0.02). The proportions of women reporting prior fracture, osteoporosis, and use of osteoporosis medication were also higher among those with VF compared with those without.
Table 1 Baseline characteristics of older women with and without any VFA-identified vertebral fracture, assessed by manual VFA or by deep learning (XVFA)The only differences between the two methods were that women with VFs identified by XVFA were shorter and more often had a family history of hip fracture, whereas women with VFs identified by the manual method had a higher prevalence of glaucoma compared with women without VFs (p < 0.05).
Associations between vertebral fractures identified by manual VFA and the risk of incident fracturesOut of 423 women, 321 (76%) had no VFs identified by VFA. Among the 102 women (24%) with any VF, 32 (8%) had a grade 1 VF, 43 (10%) had a grade 2 VF (with or without grade 1), and 27 (6%) had a grade 3 VF (with or without grade 1 or grade 2). In total, 71 women (17%) had one VF, 19 (4%) had two VFs, and 12 (3%) had three or more VFs (Tables 2 and 3). Incident fractures were categorized into four groups: any fracture, MOF, VF, and hip fracture. Associations between prevalent VFs and first incident fracture are presented in Tables 2 and 3. During a median follow-up of 7.9 years (interquartile range [IQR] 7.2–8.9) 72 women died, 138 women experienced any fracture, 102 a MOF, 44 a VF, and 30 a hip fracture. When prevalent VFs were stratified by severity, the proportion of women with any incident fracture was 47% (n = 15), 44% (n = 19), and 56% (n = 15) among those with grade 1, grade 2, and grade 3 VFs, respectively (Table 2). When stratified by number of prevalent VFs, the corresponding proportions were 48% (n = 34), 58% (n = 11), and 33% (n = 4) among women with one, two, or three or more VFs, respectively (Table 3). A similar trend was observed for incident MOF: 28% (n = 9), 37% (n = 16), and 48% (n = 13) among women with grade 1, grade 2, and grade 3 VFs, respectively, and 34% (n = 24), 53% (n = 10), and 33% (n = 4) among those with one, two, or three or more VFs, respectively. Comparable trends were also seen for incident VF and hip fracture. Incidences of fractures and death among women with any VF are presented in Supplement information 1.
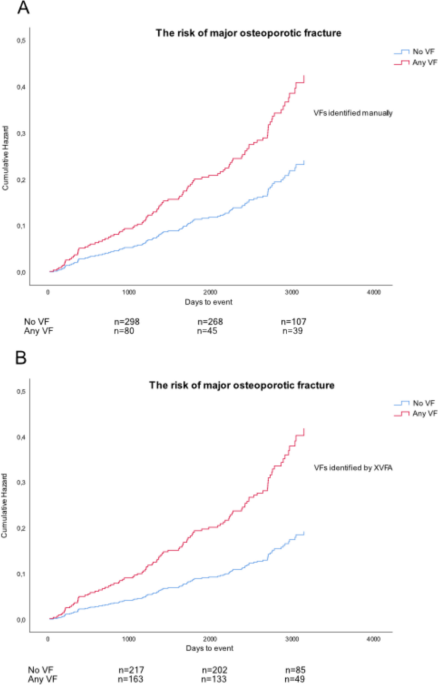
Table 2 Vertebral fracture severity and associations with subsequent fracture risk: manual VFA vs deep learning-based XVFA in older womenTable 3 Number of vertebral fractures and associations with subsequent fracture risk: manual VFA vs deep learning-based XVFA in older womenA Cox regression model adjusted for age, height, and weight revealed that having any VF identified by manual VFA was associated with an increased risk of sustaining any fracture (HR 1.99 [95% CI 1.39–2.83]), MOF (HR 2.04 [95% CI 1.35–3.07]), and VF (HR 5.30 [95% CI 2.85–9.88]). These associations were independent of CRFs included in FRAX and FN BMD (Fig. 1 and Supplement information 1). The risk of incident hip fracture was not significant (HR 1.18 [95% CI 0.54–2.60]) (Fig. 2 and Supplement information 1). When VFs were stratified by severity, having a grade 3 VF was associated with nearly a threefold increased risk of any fracture (HR 2.81 [95% CI 1.61–4.90]), more than a threefold increased risk of MOF (HR 3.41 [95% CI 1.86–6.26]), and almost a tenfold increased risk of VF (HR 9.66 [95% CI 4.46–20.94]). Stratification by number of VFs showed that having two VFs conferred an increased risk of any fracture (HR 2.98 [95% CI 1.58–5.61]), MOF (HR 3.60 [95% CI 1.83–7.10]), and VF (HR 9.56 [95% CI 4.05–22.58]). These associations remained significant after adjustment for CRFs and FN BMD (Fig. 2, Tables 2 and 3).
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Relationship between cumulative hazard for predicted major osteoporotic fracture and follow-up time (days) in older women with and without vertebral fracture (VF) at baseline, adjusted for age, height, weight, previous fracture, family history of hip fracture, current smoking, oral glucocorticoid use, rheumatoid arthritis, excessive alcohol intake, secondary osteoporosis (as used in FRAX), and femoral neck bone mineral density. In (A) VFs were identified by manual VFA; in (B) VFs were identified using the deep learning-based explainable VFA (XVFA) model
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Associations between vertebral fractures (VFs) identified by manual vertebral fracture assessment (VFA) or by the deep learning–based explainable VFA (XVFA) model and fracture risk in older women. Associations were examined using Cox proportional hazards regression models. Hazard ratios (HRs) and 95% confidence intervals (CIs) are presented in a forest plot. Clinical risk factors included previous fracture, family history of hip fracture, current smoking, oral glucocorticoid use, rheumatoid arthritis, excessive alcohol intake, and secondary osteoporosis (as used in FRAX)
Associations between vertebral fractures identified by XVFA and the risk of incident fractureOut of 423 women, 236 (56%) did not have any VFA-identified VF. Of the 187 (44%) women having any VF, 83 (20%) had a grade 1 VF, 74 (17%) had a grade 2 VF (with or without grade 1), and 30 (7%) had a grade 3 VF (with or without grade 1 VF or grade 2 VF). A total of 123 women (29%) had one VF, 43 (10%) had two VFs, and 21 (5%) had three or more VFs (Tables 2 and 3).
Associations between prevalent VFs and first incident fractures are presented in Tables 2 and 3. When VFs were categorized by severity, the proportion of women with an incident fracture was 46% (n = 38), 39% (n = 29), and 47% (n = 14) among those with grade 1, grade 2, and grade 3 VFs, respectively (Table 2). When categorized by number, the corresponding proportions were 39% (n = 48), 49% (n = 21), and 57% (n = 12) in women with one, two, or three or more VFs, respectively (Table 3). A similar trend was observed for incident MOFs: 36% (n = 30), 28% (n = 21), and 43% (n = 13) in women with grade 1, grade 2, and grade 3 VFs, and 29% (n = 35), 40% (n = 17), and 57% (n = 12) in women with one, two, or three or more VFs, respectively. Similar patterns were also seen for incident VFs and hip fractures (Tables 2 and 3). Incidences of fractures, deaths, and time at risk among women with any VF are presented in Supplement information 1.
A Cox regression model adjusted for age, height, and weight revealed that the presence of any XVFA-identified VF was associated with an increased risk of incident any fracture (HR 2.04 [95% CI 1.44–2.87]), MOF (HR 2.32 [95% CI 1.55–3.48]), VF (HR 4.21 [95% CI 2.06–8.59]), and hip fracture (HR 2.93 [95% CI 1.33–6.44]). These associations were independent of CRFs included in FRAX and FN BMD (Fig. 1 and Supplement information 1).
When XVFA-identified VFs were stratified by severity, the presence of a grade 3 VF was associated with more than a twofold increased risk of any fracture (HR 2.39 [95% CI 1.32–4.31), a more than threefold increased risk of MOF (HR 3.31 [95% CI 1.75–6.26]), an over eightfold increased risk of VF (HR 8.55 [95% CI 3.53–20.75]), and an almost fivefold increased risk of hip fracture (HR 4.70 [95% CI 1.57–14.20]) (Table 2).
When VFs were categorized by number, the risk of any fracture, MOF, VF, and hip fracture among participants with three or more VFs was even higher (HR 3.89 [95% CI 2.06–7.34], HR 6.29 [95% CI 3.24–12.21], HR 13.49 [95% CI 5.39–33.75], and HR 6.06 [95% CI 1.83–20.14], respectively) (Table 3). These associations remained robust after further adjustment for CRFs and FN BMD (Fig. 2, Tables 2 and 3).
Incident non-vertebral fracturesAdditional analyses were conducted for incident non-vertebral fractures. Overall, no consistent associations were observed between VFs, whether identified by XVFA or manual VFA, and the risk of incident non-vertebral fractures. One isolated association was observed for grade 1 VFs identified by XVFA after adjustment for CRFs (HR 1.69, 95% CI 1.02–2.80), which should be interpreted with caution given the number of comparisons performed. Detailed results are presented in Supplement information 2.
Kaplan–Meier survival analysis for fracture predictionDue to differences in the number of women with prevalent VFs identified by manual VFA and XVFA, a Kaplan–Meier survival analysis was performed for four groups based on baseline VF status: both negative (n = 217), manual only (n = 19), XVFA only (n = 104), and both positive (n = 83) (Fig. 3). The agreement between methods was fair (κ = 0.38). Figure 3 shows Kaplan–Meier curves for incident fracture–free survival across these groups. Participants with VFs identified by both methods had the highest incidence of subsequent fractures, while those without VFs by either method had the lowest risk. Individuals with VFs detected by only one method showed intermediate risk levels. Censoring was appropriately accounted for in the analysis. Notably, participants with VFs detected by XVFA but not by manual VFA (n = 104) showed divergence in fracture incidence compared with participants with no VFs. The global log-rank test across all four groups was statistically significant (p < 0.001). In pairwise comparisons, the XVFA-only group differed significantly from the no-VF group (log-rank p < 0.001), indicating that XVFA may capture prognostically relevant fracture risk. In multivariable Cox regression adjusted for CRFs and FN BMD, the association remained statistically significant (HR 2.23, 95% CI 1.45–3.43, p < 0.001).
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier survival curves for incident fractures in the held-out test set (total n = 423), stratified by baseline vertebral fracture status assessed by manual VFA and XVFA. Groups were: both negative (n = 217, blue), manual only (n = 19, red), XVFA only (n = 104, green), and both positive (n = 83, orange). Censoring is accounted for but not shown for clarity. XVFA = explainable vertebral fracture assessment (a model developed using deep learning)
Comments (0)