
Remember me
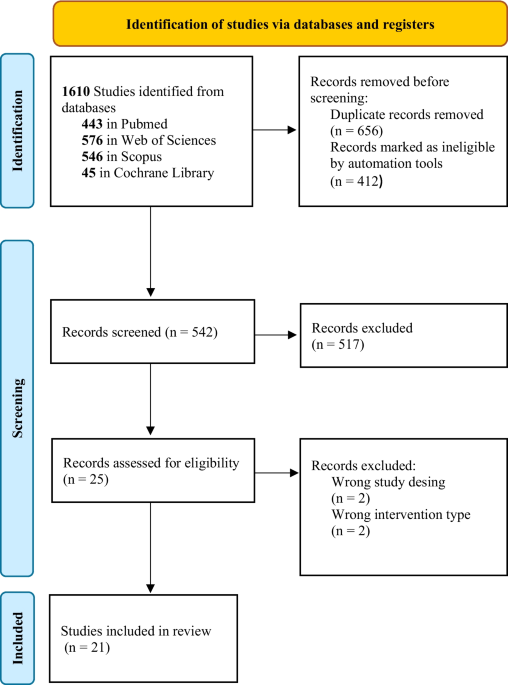
In the original search, a total of 1610 articles were identified, of which 656 duplicates were removed and 412 were excluded using a reference management tool. Finally, a total of 21 articles were included in this systematic review based on the previously established inclusion criteria. The selection process is presented in Fig. 1.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.PRISMA flowchart of the systematic review process
Characteristics of the included studiesThe main characteristics of the included studies are described in Table 1. The studies consisted of randomized controlled trials, except for three quasi-experimental studies [27,28,29] and a pilot study [30]. All the included studies were published between 1998 [31] and 2024 [32], with most conducted in Northern Europe, followed by Australia, the USA, and Asia. The total sample consisted of 2076 participants, with a mean age (± standard deviation) of 72.77 (± 5.57) years.
Table 1 Characteristics of the included studiesMost studies included only women in their samples, except for six [27, 30, 32,33,34, 45] that included both male and female participants. The time from fracture to study inclusion varied, with some studies not specifying a timeframe, while others required the fracture to have occurred at least 3 months [30, 34, 44, 45] or at least 6 months [29, 36,37,38, 40] before the intervention.
In regard to the included outcomes and assessment tools, functional capacity was the most evaluated domain, measured in 14 studies (66.7%). The Timed Up and Go (TUG) test was the predominant instrument within this domain, employed in 11 studies [28, 31, 33,34,35, 37,38,39, 41, 44, 47]. Self-reported pain was the second most frequent outcome, assessed in 12 studies (57.1%), with the Visual Analogue Scale (VAS) being the most common tool, used in 9 studies [28, 29, 34, 35, 37,38,39,40,41]. Quality of life was evaluated in 11 studies (52.4%), where the QUALEFFO-41 questionnaire was the instrument of choice in 8 instances [30, 33,34,35, 37, 38, 45, 46]. Other domains were quantified less frequently: balance was assessed in 10 studies (47.6%), thoracic posture in 8 studies (38.1%), trunk muscle endurance in 6 studies (28.6%), and aerobic capacity in 5 studies (23.8%). These domains utilized a wider variety of specific tests, indicating a lower degree of standardization for these particular outcomes.
Regarding the types of interventions, two studies focused exclusively on health education programs [27, 32]. Most interventions focused on multicomponent physical exercise programs. A total of six studies focused their physical exercise programs on core strength and motor control combined with aerobic training [29, 33, 35, 36, 43, 44], while two studies added resistance training to the abovementioned components [38, 39] and only one study combined all four elements: core strength, motor control, resistance, and aerobic exercise [28]. Seven of them included only core strength and motor control [31, 34, 37, 40,41,42, 47]. Two of the included studies combined resistance and aerobic exercise [45, 46] and finally, one physical exercise program focused on mindfulness and yoga [30]. To summarize, the most common interventions were those targeting core strength and motor control (35%), followed by core strength, motor control, and aerobic programs (30%), resistance and aerobic programs (10%), core strength, motor control, resistance, and aerobic exercise (5%), and mindfulness and yoga (5%).
Risk of biasTables A.2, A.3, and A.4 show the assessment of risk of bias. One of the included studies was not assessed because the full text was not available, so data were not sufficient to complete the assessment [47].
Among the 17 randomized controlled trials included, 14 (82%) presented a low risk of bias and 3 (18%) showed a high risk of bias. The main sources of bias were related to the blinding of outcome evaluators, the identification and control of potential confounders, and the reporting of per-protocol and intention-to-treat analyses. Most studies reliably measured outcomes (82%) and performed appropriate statistical analyses (88%), also providing adequate information on randomization procedures and baseline comparability between groups. As for the quasi-experimental studies, two were rated as low risk of bias and one as moderate. These studies met most of the quality criteria, except for participant inclusion (66%), group differences before the intervention, and the appropriate use of statistical analysis, which was only fulfilled by one study (33%). Overall, the quasi-experimental studies demonstrated acceptable methodological quality, though further improvement is needed in reporting baseline comparability and statistical analyses.
Effectiveness of exercise on functional and aerobic capacity, balance, trunk muscle strength/endurance, and quality of lifeA total of 16 trials [28, 29, 31, 33,34,35,36,37,38,39,40, 42, 44,45,46,47] evaluated the effects of physical exercise on desired outcomes. Ten studies assessed functional capacity, 4 evaluated aerobic exercise capacity, 10 of them evaluated balance, 7 analyzed trunk muscle strength/endurance, and 9 trials evaluated quality of life. Analyses by study level showed a significant heterogeneity, except for aerobic exercise capacity, and balance (I2 = 0%, 44% and 0%, respectively). Considering all the included studies, we found more favorable results for the physical exercise interventions in terms of functional capacity (SMD −0.41; 95% CI −0.69, −0.14), aerobic exercise capacity (SMD 25.29; 95% CI 5.33, 45.26), balance (SMD 0.35; 95% CI 0.16, 0.53), trunk muscle strength/endurance (SMD 0.69; 95% CI 0.22, 1.16), and quality of life (SMD 0.48; 95% CI 0.13, 0.82). All results are shown in Fig. 2. No publications bias was detected in any analysis (Figure A.1). Results were robust for all variables except aerobic exercise capacity, which lost statistical significance after removing the study by Marini, S. et al. [28] (Table A.5). Meta-regression analyses showed that some moderators influenced the effects of exercise interventions. Functional capacity was better in younger patients than in older ones (β = 0.14; p = 0.020). The effects on balance were better with multicomponent interventions (core stability, motor control, resistance training, and aerobic) compared to less comprehensive or unsupervised home interventions (β = 0.20; p = 0.031). Aerobic exercise capacity and quality of life were not affected by any moderator (p > 0.050).
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Pooled standardized mean difference for the change in desired outcomes functional capacity, aerobic exercise capacity, balance, trunk muscle strength/endurance, and quality of life. TUG Timed Up and Go, 30CTS 30-s Chair Stand Test, SPPB Short Physical Performance Battery, TLS Time Loaded Standing, QUALEFFO-41 41-Item Quality of Life Questionnaire of the European Foundation for Osteoporosis, EQ-5D EuroQol instrument, SF-36 36-Item Short Form Health Survey
Effects of exercise on thoracic posture and pain
Comments (0)