
Remember me
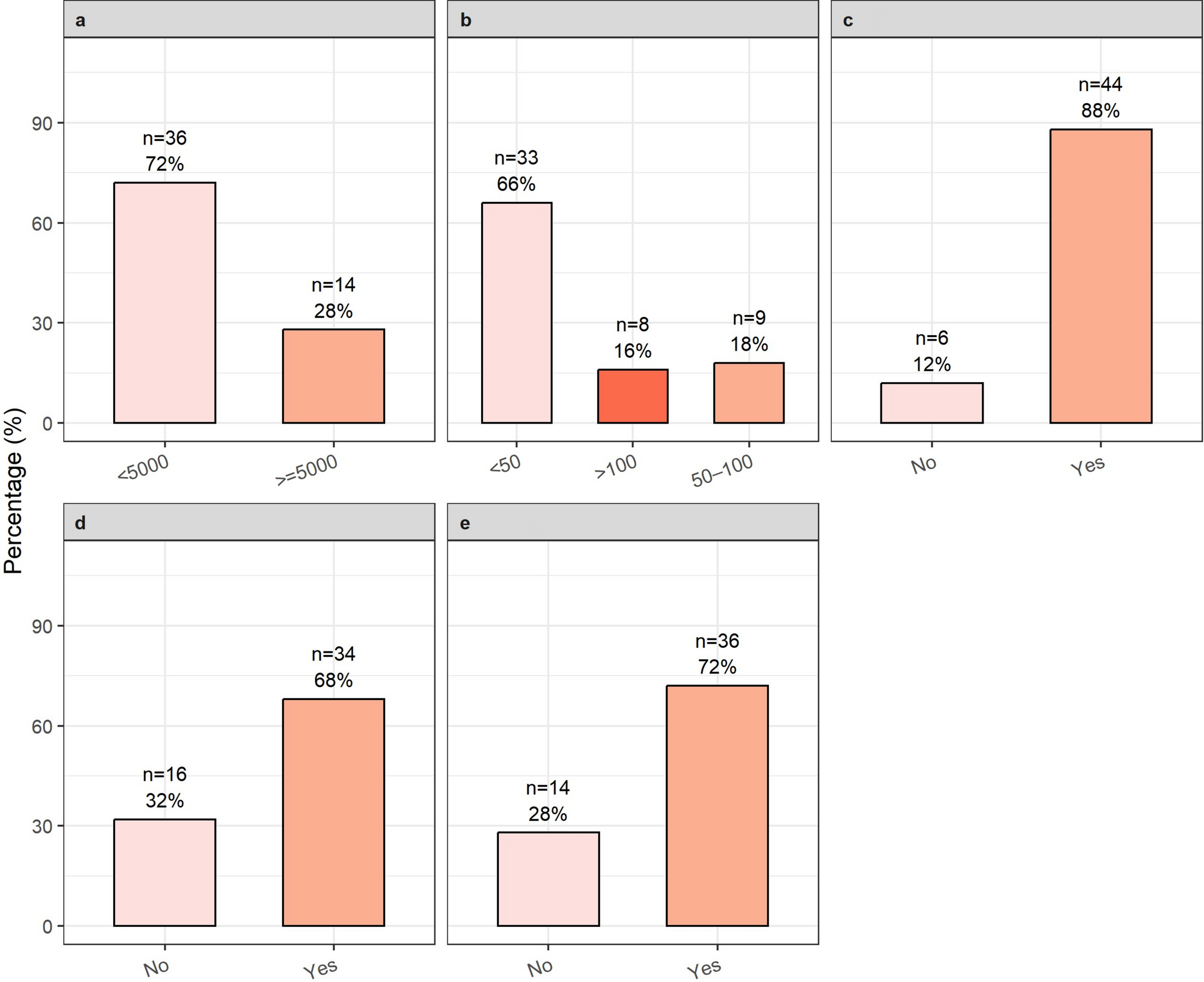
Thirty-four responses were received from physical activity providers (22 PE teachers, 10 sports coaches, and 2 outdoor activity supervisors) who supported adolescents (12–18 years) in physical activity. Descriptive characteristics of survey respondents are shown in Table 1. The respondents included a mix of males (n = 19) and females (n = 15). Years of experience in roles ranged from 1 to 38 years (median of 7 years). Eight participants had personal experience of T1D, with either themselves or family members having the condition.
Table 1 Characteristics of survey participantsOnly four respondents (11%) said they were aware of their school/club having a policy for supporting children and adolescents with T1D. This was substantially lower than for other chronic conditions (n = 10, 30%) such as epilepsy, asthma, and allergies.
Physical activity provider confidence in supporting physical activityPhysical activity providers’ confidence in supporting aspects of diabetes management around physical activity is shown in Table 2. Only half of respondents (n = 17) felt confident or very confident in supporting children and adolescents with T1D to engage in physical activity. Less than half (n = 14) were confident with pre-exercise blood glucose checks or with pre-exercise carbohydrate intake, and less than a third (n = 10) with pre-exercise insulin adjustment. Only around a quarter (n = 9) felt confident or very confident in dealing with a diabetic emergency. Just over half (n = 19) of respondents felt confident adapting sessions to be inclusive for children and adolescents with T1D.
Table 2 Physical activity providers confidence in supporting physical activity in children and adolescents with T1DKnowledge about T1D and training needsTwo-thirds (n = − 23/34) rated their knowledge of T1D as average or below. Of the eleven respondents with good or excellent knowledge, eight participants had personal experience of T1D. Most (n = 29/34) felt it would be very important or important to develop training materials for helping physical activity providers to support children and adolescents with T1D to be physically active with almost all (n = 32/34) saying they would make use of any training resource.
Thirty respondents had received formal training for their role but only ten had received any sort of training relating to T1D. Formal training relating to the role included degrees and teaching qualifications for teachers, and coaching qualifications for sports coaches (for example ‘FA level 1 Coaching’) Training relating to T1D most commonly as part of routine first aid training (n = 3/10) or informally through school nurses (n = 3/10), charities (n = 1/10), parents (n = 1/10), or hospital staff (n = 1/10). Training was more common among PE teachers (n = 7/22) than sports coaches and two outdoor activity supervisors (n = 2/12).
Semi-structured interviewsSample characteristicsNine physical activity providers supporting adolescents were interviewed, including four PE teachers and five sports coaches. Participants had been in their respective roles for 5 or less years, 6 to 10 years, or more than 10 years. Characteristics of participants are shown in Table 3. Of the four PE teachers, two were independent schools, two state schools. The Sports coaches were involved in supporting a range of sports with specific experience of supporting rugby, football, netball, volleyball, and rowing. Participants were located across the UK, with participants in Scotland (n = 2), Wales (n = 2), and six in England (Southwest (n = 2), Southeast (n = 2), West midlands (n = 2)). All but one of the sports coaches interviewed were involved in a voluntary manner.
Table 3 Characteristics of interview participantsSurvey responses from interview participants indicated that eight of the nine participants felt confident or very confident in supporting an adolescent with T1D to engage in physical activity. Four of the participants had some direct lived experience of T1D either having the condition themselves (n = 1), a partner (n = 1) or their child (n = 2).
Factors influencing physical activity supportOur findings fit into two overarching categories; the current context in which physical activity providers work and strategies for providing support that take account of the current context. Findings from interviews are summarised in Fig. 1. Verbatim quotes are provided to demonstrate themes, labelled with the participant’s role.
Fig. 1
Summary of key categories and themes
Current contextPhysical activity providers fulfil various roles and therefore require a range of training and practices. Through the interviews, participants shared relevant experiences regarding the current resources, guidelines, and practices available to them or lack thereof when supporting children and adolescents with T1D.
Limited access to T1D training and resourcesInterview participants indicated that they had received little to no formal training on T1D, particularly in terms of supporting children and adolescents with the condition or understanding how physical activity might impact its management. The little formal training some had received was through first aid qualifications which covered basics of hypoglycaemia. Instead, physical activity providers cited others with personal experience as their source of knowledge/education. Participants suggested that knowledge within clubs and schools is dependent on a member of staff having T1D or being a parent of a child with T1D.
‘We have no formal training on diabetes, how it affects, and specifically how it affects children throughout the school day’ (Participant 2, PE teacher)
The physical activity providers interviewed believed this lack of training and experience has a direct impact on their ability to provide sufficient support. This introduces an element of luck as the chances of a child or adolescent with T1D receiving appropriate support is based on their physical activity providers personal experiences and motivation to gain understanding.
‘The schools know a little bit, but no one knows huge amounts unless you happen to have a teacher in the school whose children got diabetes’ (Participant 4, PE teacher)
Lack of policy and guidanceSeveral interview participants described not being aware of any policies or guidance for managing and supporting children and adolescents with T1D within their school or club. As a result, it was apparent that some participants were not always made aware of children and adolescents in their school or club who had a T1D diagnosis. It was suggested that this may result from fear of breaking confidentiality meaning information was not passed to potentially appropriate members of staff, including passing on information about other medical conditions.
‘We’ve not got guidance in school that I’m aware of’ (Participant 4, PE teacher)
‘The club don’t really have anything in place for that now that I think about it’ (Participant 5, Sports coach)
Reactive rather than proactive educationDue to limited time and limited policies for mandated training, it was indicated that education around T1D was reactive to encountering a child with T1D and initiated by the physical activity providers themselves. Physical activity providers described searching for resources after discovering a child or adolescent with T1D was in their club or class. This was not always successful with some describing difficulties finding appropriate resources.
‘There were three or four [Physical activity providers], they wanted to know about diabetes, they wanted to learn. I think one of the students got diagnosed during their watch and they wanted to find out a lot about it.’ (Participant 8, Sports coach)
Coping strategies used to support children and adolescents with T1DThe lack of policy and training available to providers resulted in a range of coping strategies. These approaches fall under three broad themes, communication, responsibility, and practical steps, as outlined below.
Communication about needsPhysical activity providers often relied upon the YP’s family and/or diabetes clinical team to gain knowledge and specific guidance for supporting each child. It was felt that communication was essential in building trust with both the child with T1D and their parents. Physical activity providers also emphasised the importance of the child or adolescent with T1D as a source of diabetes education.
‘The students have always been very, very educated themselves … they are the educators’ (Participant 2, PE teacher)
In addition, physical activity providers described communication as being an important strategy in itself for supporting children and adolescents, checking in during sessions and prompting them to check their blood sugars.
‘That’s the thing that’s come across to me when I’ve had those conversations with parents. It’s about 5 or 10 min into the conversation they often visibly relax cause they’re like, OK, this person has obviously dealt with this before and has an understanding and isn’t just flippant… and that kind of stuff is good for reassuring a parent’ (Participant 9, Sports coach)
Responsibility placed on childWithout clear policy, physical activity providers explained there was no accountability for them to provide support, so the responsibility during activities was often left to the child or parents who would be present to supervise in the case of sports clubs. There was also an expectation for students to communicate their concerns and needs for them to receive adequate support. Physical activity providers also raised concerns that a child or adolescent with T1D may not discuss their glucose levels with them due to embarrassment or fears of letting staff down.
‘When they go on to first year at the age of 12, they’re classed as young adults, so there’s no one there to support them, so there’s no information given, so they’re kind of expected to just deal with that on their own’ (Participant 7, PE teacher)
Ensuring access to diabetes equipment and use of technologyParticipants described how equipment and technology aided activity sessions. Continuous glucose monitors (CGMs) were utilised throughout sessions and were particularly helpful for students who struggled to keep track of glucose changes and communicate those changes to their physical activity provider. Some participants raised potential problems with CGMs, for example, the technology failing or the inability to communicate blood glucose levels without phone signal. Other participants described how, for certain sports, CGMs may cause barriers to participation for children and adolescents with T1D.
‘because of the sensor we were able to have his phone on the poolside and every 15 min check it so that we didn’t have to rely on him being the person to tell us because he was rubbish at communicating…so it made it much more accessible in order to be able to look after him so that he could actually access all of his lessons’ (Participant 2, PE teacher)
Other equipment utilised by coaches and teachers for children and adolescents with T1D included various forms of dextrose and glycogen packed in a bag to be carried by the individual or coach throughout the session in case of emergency. One coach referred to having duplicates of this ‘diabetes kit’ (hypo treatment) for staff.
‘-we carry one of them [glucose shots] in each of the launches’ ‘I try and remember if they’re going out for a head race or something along those lines, that the cox takes some sweets with him’ (Participant 1, Sports coach)
‘My first question was always where do you keep your sugar supply? And so then I was like, right, it would actually be a good idea for me to have a bag with all this stuff in and for the kids to have a bag. And so we always have a duplicate of that just to make sure’ (Participant 9, Sports coach)
Recognising individual differencesAnother factor highlighted was that different children and adolescents want and require different support. This individual variability adds a layer of complexity for physical activity providers trying to provide support.
‘I really struggle supporting young people with Type 1 Diabetes, and it’s very much you get that attitude ‘oh well we have one child with Type 1 so we kind of know what we’re doing’ but actually no you don’t because every child’s different.’ (Participant 7, PE teacher)
Physical activity providers faced the dilemma of whether to take precautions to protect the YP with T1D or treat them the same as any other child. Some physical activity providers were quite clear that they did not adapt the session; however, this was not always the case, with one participant recognising that a YP with T1D wanted to avoid certain movements due to their glucose monitor and insulin pump. Some children and adolescents were described as independent in managing their condition, but for others, their peers had to prompt them to manage their blood glucose or help them to identify when blood glucose levels were falling low. One teacher mentioned their concerns around supporting students with both T1D and communication challenges.
‘What I’ve gathered from the lads I’ve looked after in the past is they’re different. They’re not all, you know, one case isn’t the same as another case in terms of how they manage it and how they’re comfortable with managing it’ (Participant 2, PE teacher)
Comments (0)