Globally, neonatal sepsis is a major health issue, characterized by systemic infection with bacteremia within 28 days after birth [1]. Still, a key factor of death and morbidity in neonatal intensive care units (NICU) all over is this illness [2, 3].
The surgical neonates are more prone to infection due to invasive procedures and contact with pathogenic bacteria in the hospital environment. Availability of better antibiotics has reduced deaths due to infection, but sepsis is still a significant cause of death among newborn surgical patients [4].
While antibiotic intervention is essential, it presents its own challenges, potentially leading to adverse outcomes in uninfected infants [5,6,7]. This has prompted an investigation into novel diagnostic approaches and therapeutic strategies [8]. Vitamin supplementation, particularly vitamin C, has garnered significant attention among these emerging interventions. Vitamin C, an essential micronutrient, demonstrates promising potential in sepsis management through its diverse biological functions [9].
Recent research has revealed that critically ill septic patients typically present with depleted vitamin C levels, corresponding with rising organ malfunction and death [10]. The therapeutic potential of vitamin C in sepsis is attributed to its multifaceted mechanisms, including its role as an enzymatic cofactor in catecholamine and cortisol production [11], its antioxidant properties in managing reactive oxygen species [12], and its ability to preserve capillary blood flow and vasoactive medication–induced vascular responsiveness [13].
This study aims to evaluate the effectiveness of intravenous (IV) vitamin C for septic neonates, mechanically ventilated (MV) full-term neonates following surgical interventions, specifically examining its impact on ventilation parameters, weaning time, and inotropic support requirements.
Patients and methods.
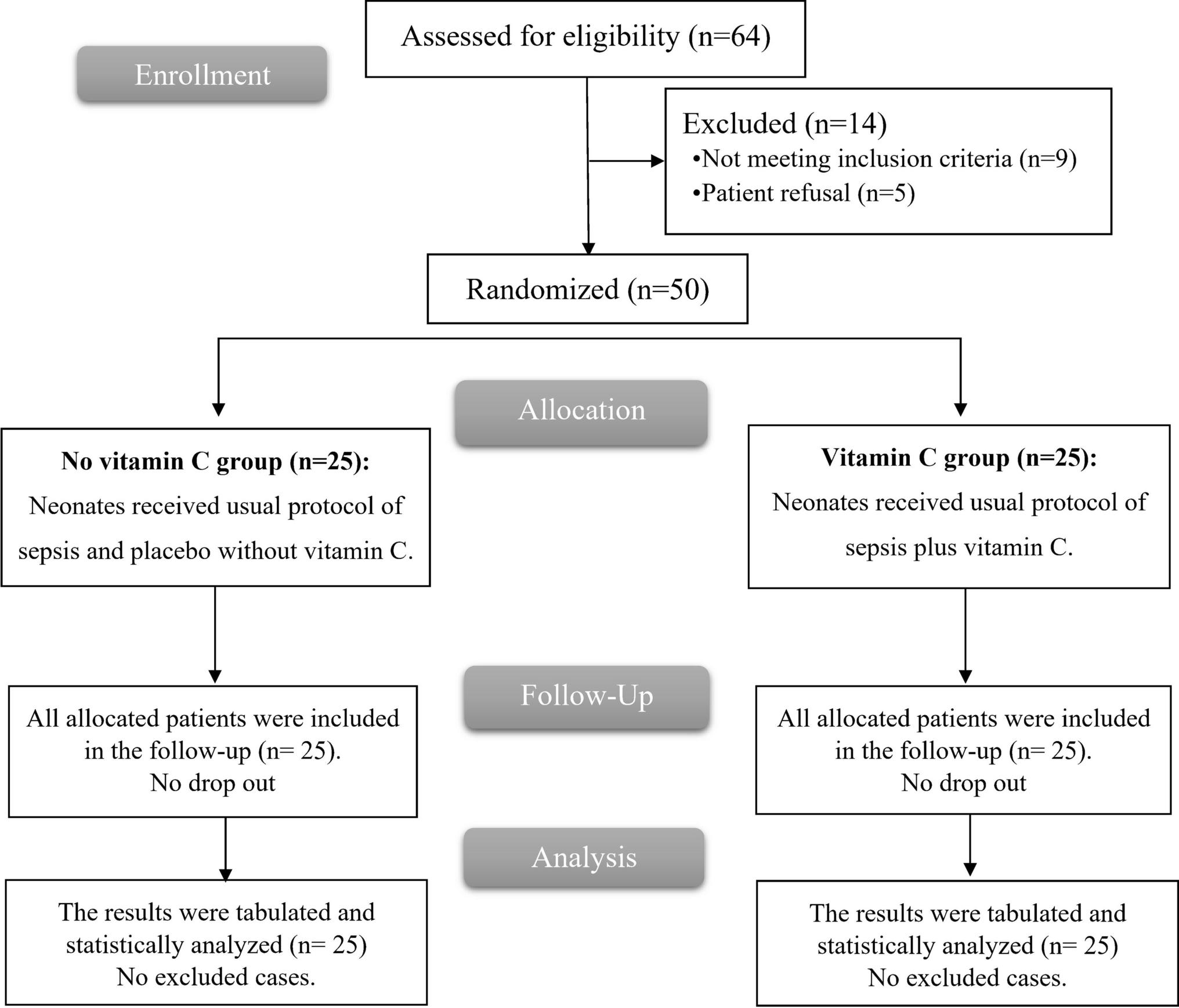
This double-blinded randomized controlled trial included 50 full-term neonates (gestational age > 37 weeks) who required MV and developed clinically and serologically confirmed sepsis after undergoing surgical procedures. The study was conducted in the NICU at Tanta University Hospital, Egypt, from February 2023 to August 2023. The trial was approved by the institutional ethics committee (approval ID: 36264PR117/2/23), was done in accordance with the Declaration of Helsinki, and was registered on ClinicalTrials.gov (ID: NCT06780345) (date: 17/1/2025). Written informed consent was obtained from all participating neonates’ parents or legal guardians.
Neonates were excluded from the study if they presented with major congenital anomalies or chromosomal abnormalities or were born at a gestational age of less than 37 weeks. Additional exclusion criteria included the presence of hypoxic ischemic encephalopathy, neuromuscular diseases, or intraventricular hemorrhage.
Randomization and blindness
Using computer-generated random numbers, neonates were divided into two equal groups (using https://www.randomizer.org/) in sealed opaque envelopes. No Vitamin C group (control group), who received the standard sepsis management protocol with a placebo, and Vitamin C group, who received the standard protocol along with a vitamin C infusion, administered as a 0.5 g/kg loading dose followed by a maintenance dose of 0.5 g/kg/h over 6 h, continued for 7 to 10 days [14].
The attending NICU physicians responsible for data collection and the parents or guardians of the neonates were blinded to the group allocation and the treatment administered.
All enrolled neonates underwent a comprehensive evaluation, including history-taking and a thorough clinical examination. Laboratory investigations comprised a complete blood count, liver function tests, blood urea nitrogen, creatinine levels, arterial blood gas analysis, and C-reactive protein measurement.
Study parameters, including mean arterial blood pressure (MAP), heart rate (HR), and arterial oxygen saturation (SpO₂), were continuously monitored in both groups. Mechanical ventilation parameters, including respiratory rate (RR), peak inspiratory pressure (PIP), and fraction of inspired oxygen (FiO₂), were recorded at baseline, 24 h, 72 h, and 120 h following the initiation of the infusion.
The need for inotropic support was documented. The total duration of MV was recorded at discharge, along with the length of hospital stay and mortality outcomes.
The primary outcome was the duration of MV. Secondary outcomes included the need for inotropic support and mortality rates.
Sample size calculation
G*Power 3.1.9.2 (Universität Kiel, Germany) was used to calculate the sample size. A pilot study, including five cases in each group, revealed that the mean (± standard deviation) duration of MV was 6.6 ± 1.95 days in the study group and 8.6 ± 1.52 days in the control group. The sample size determination was based on an effect size of 1.14, a 95% confidence level, and a study power of 95%, with an equal allocation ratio (1:1) between groups. Additionally, four participants were added to each group to account for potential dropouts. Consequently, a total of 25 patients will be recruited per group.
Statistical analysis
We used SPSS version 27 (IBM©, Armonk, NY, USA) for statistical analysis. The Shapiro–Wilk test and histograms were used to determine whether the data distribution was normal. Mean and standard deviation (SD) were used to present quantitative parametric data, which were examined using the unpaired Student’s t-test. For qualitative variables, frequency and percentage were used for description, and the chi-square or Fisher’s exact test was used for evaluation, as appropriate. Statistical significance was determined by a two-tailed p value less than 0.05.

Comments (0)