This multi-center study provides a comprehensive analysis of RSV hospitalizations in children during their second year of life over four consecutive seasons (2017–2021). Comparing hospitalization outcomes between children with and without individual risk factors, specifically prematurity, CLD of prematurity, CHD, and DS revealed that RSV infection remains a significant threat for these high-risk groups during their second year of life. This is reflected in the increased severity of RSV hospitalizations, as evidenced by higher rates of prolonged LOS (LOS > 3 days) across all high-risk groups and higher rates of PICU admissions among those with ≥ 1 of these risk factors. Children with DS and major CHD were also associated with higher rates of PICU admissions, but this finding should be interpreted cautiously given the relatively limited number of cases.
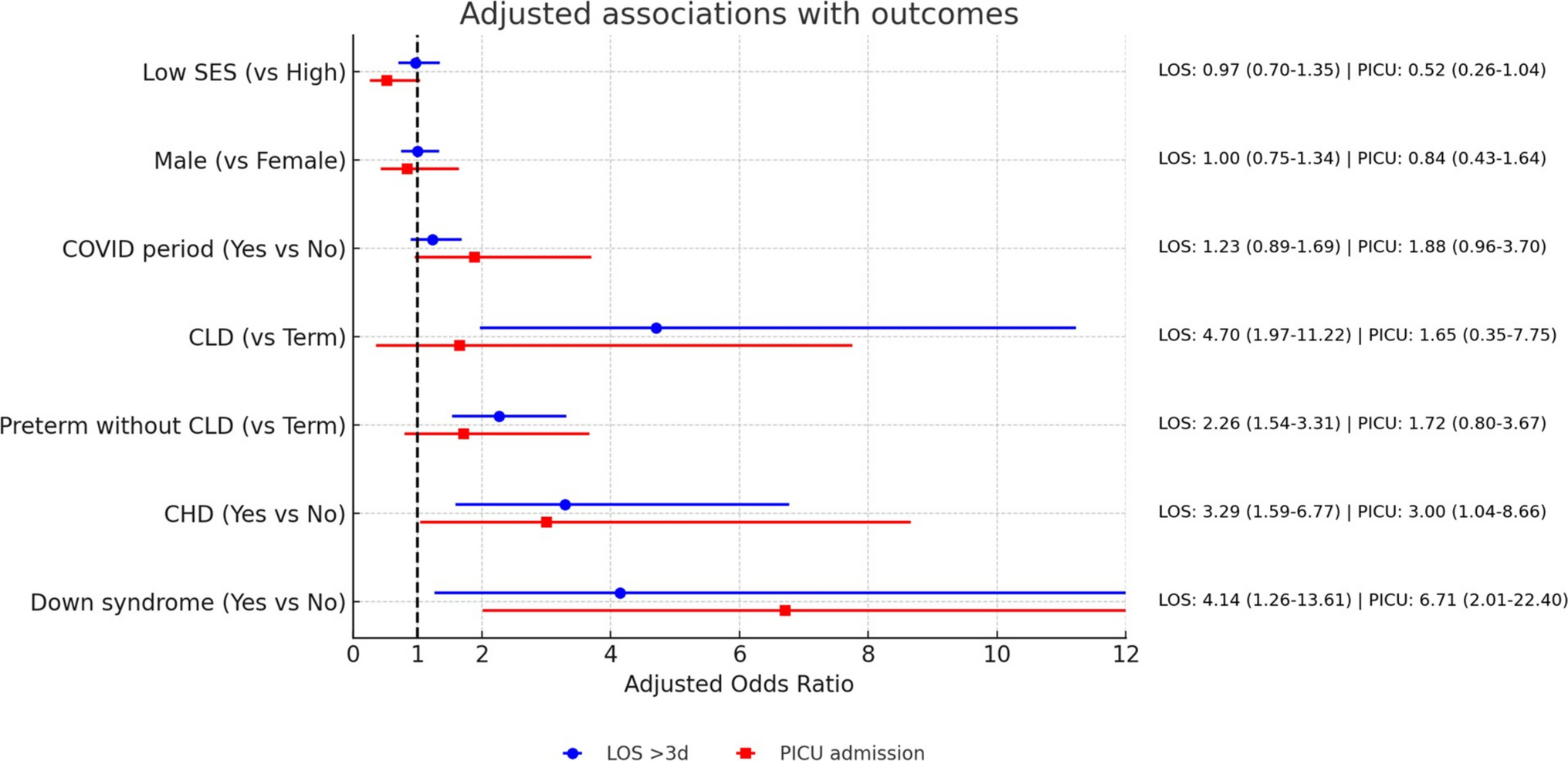
Our study found that children born premature had 2.6-fold higher rates of prolonged hospital stay and twofold increased risk of PICU admission compared with term children. Furthermore, gestational age. whether analyzed as a continuous variable or by subgroups of early and late preterm was significantly associated with prolonged length of stay. Notably, even after adjusting for potential confounders in the multivariable analysis, prematurity remained a strong independent predictor for prolonged hospitalization, with preterm infants without CLD showing more than a twofold increase in risk and those with CLD nearly a fivefold increase compared with term children. Although preterm infants are recognized as being at risk for severe RSV infections beyond their first year of life, the extent of this risk varies across studies. Several reports have shown that early preterm children (< 32 wGA) have more than twice the risk of RSV-associated hospitalization in their second year compared to the general infant population. Findings on late preterm children (33–36 wGA) remain inconsistent. Wang et al. reported risks similar to term infants, whereas Helfrich et al. found that even healthy late preterm infants had nearly double the hospitalization risk in their second year. Unlike our study, however, these analyses did not provide detailed outcome data during the second year of life,[11].[18]. Several mechanisms described in the literature may contribute to the prolonged vulnerability of children born premature to severe RSV [19]. Preterm children exhibit impaired lung function, including airway obstruction and reduced elasticity. Although some improvement occurs during the second year of life, lung function in preterm infants often continues to lag behind that of their term-born peers [9]. This persistent impairment is thought to result from dysanaptic lung growth and early-life exposures such as mechanical ventilation and oxygen toxicity [20, 21].
Children with DS in our study had a more severe hospital courses, with at least a fourfold higher risk of prolonged hospitalization compared with patients without DS. In the multivariable analysis, they also showed higher odds of PICU admission (OR 6.7, 95% CI 2.01–22.4); however, the wide confidence interval reflects the limited sample size, so this finding should be considered exploratory and requires confirmation in larger studies. The severe hospital course is likely attributable to multiple factors, including potential airway malformations, comorbidities, and significant immunologic dysregulation affecting both innate and adaptive immunity of patient with DS [22]. Our findings regarding DS patients, are in line with previous studies [9]. [23] [24] Megged et al. found that patients with DS admitted with RSV were significantly older than healthy children. Specifically, 41% of them were older than one year of age, and 20% remained at high risk for a severe course of illness even beyond the first two years of life [23]. A meta-analysis of 12 studies across 10 countries reported that children with DS infected with RSV had an 8.7-fold increased risk of hospitalization and a 2.7-fold increased risk of PICU admission. Their average hospital stay was 4.7 days longer as compared with children without DS [24]. However, the studies included in the meta-analysis provided limited age-specific analysis.
Children with major CHD had a threefold higher adjusted risk of prolonged hospitalization and PICU admission. These findings align with prior studies, including a large U.S. inpatient database, showing RSV remains a substantial risk for children with hemodynamically significant CHD into the second year of life [25, 26] This population has been shown to face an increased likelihood of RSV-related hospitalization, prolonged hospital stays, mechanical ventilation, and mortality, with certain subgroups being at even higher risk of mortality [26]. In our cohort, children with CHD and also those with ≥ 1 risk factor were older at the time of RSV hospitalization. This suggests that their vulnerability extends further into the second year of life. Similarily, previous studies from Israel, Australia, and the United States, demonstrated that children hospitalized with RSV and comorbidities tend to be older than their healthy counterparts. [9, 27,28,29,30] The overall clinical course was more severe among children with at least one risk factor compared to those without, as reflected by a 3.5-fold increased risk of both prolonged hospitalization and PICU admission. While Shmueli et al. also reported increased severity of RSV-related hospitalization outcomes among children under two years with chronic diseases, only a small proportion of their cohort (94 out of 1,124) were aged 12–23 months. In contrast, our study offers a more targeted insight into this specific age group.
In our study, children from higher-SES families had shorter RSV hospital stays. This finding is consistent with previous reports linking higher SES to earlier presentation and reduced LOS, whereas lower SES has been associated with greater RSV hospitalization risk and illness severity. These disparities likely reflect differences in healthcare access and health literacy, underscoring the importance of equitable prevention strategies. [31,32,33]
RSV immunoprophylaxis recommendations for children aged 12–23 months vary worldwide. The AAP recommends nirsevimab only for selected high-risk 8–19 months infants with CLD requiring recent support, severe immunocompromise, or severe CF, but not for DS, prematurity, or CHD alone. In contrast, countries such as Switzerland have adopted broader criteria, recommending prophylaxis for children with persistent high-risk conditions, including significant CHD, DS, or prematurity < 33 weeks. These differences reflect variations in health systems, risk assessment, and evolving evidence on nirsevimab’s efficacy in older children. [34].[35]
A major strength of our study is the use of comprehensive data from a large cohort of children across multiple medical centers. Another strength of our study is the laboratory-confirmation of RSV. In contrast, some previous studies used RSV-codes to identify RSV hospitalization, which are known to underestimate the true rate of RSV-related hospitalizations [9, 36, 37]. Importantly, our study focuses on a highly relevant population, children hospitalized with laboratory-confirmed RSV disease during their second year of life who are expected to continue to play a substantial role in the RSV burden for the coming years.
The present study's limitations include its retrospective design. We also focused on specific documented risk factors, but unmeasured comorbidities, such as cystic fibrosis, severe immunosuppression, neuromuscular disorders, and other genetic syndromes may also affect RSV hospitalization severity outcomes. Importantly, our multivariable analysis demonstrated that the specific risk factors we examined remained significant after adjusting for potential confounders. Another limitation is the lack of patient-level data on the status of surgical correction for patients with CHD, which may have affected their risk profile as well as the grouping of CHD diagnoses together. However, the study was restricted to specific major CHD cases with hemodynamic significance, which typically require corrective or palliative surgery in the first year of life. Thus, the impact of this limitation is likely reduced. Furthermore, we were unable to collect individual data on palivizumab administration among children with CLD of prematurity. However, large multicenter cohort studies confirm that fewer than 2% remain oxygen dependent beyond the first year of life, [38,39,40] suggesting that palivizumab prophylaxis in our cohort was likely limited. Nevertheless, if any did receive prophylaxis, the risks we observed may underestimate the true burden of severe RSV in this population.
Moreover, we also appreciate that our study includes data from 11 different medical centers and therefore variability across sites regarding admission thresholds could have affected our results. Another limitation is that RSV hospitalizations were identified by laboratory confirmation rather than ICD-10 codes, possibly causing overlap with other RSV-related diagnoses (e.g., pneumonia, wheezing illness, or potential nosocomial infection). However, limiting the analysis to each child’s first RSV-positive hospitalization likely captured the primary illness leading to admission, which in this age group is typically bronchiolitis. Lastly, the study period included the COVID-19 pandemic, which disrupted RSV seasonality [41]. However, we assessed its potential impact in our multivariable analysis and found no significant effect of the pandemic on RSV hospitalization outcomes. This suggests that host factors and underlying comorbidities may play a more central role in determining disease severity than timing of circulation.
In conclusion, children hospitalized with RSV in their second year of life with prematurity, CLD, CHD, or DS experienced significantly more severe disease outcomes reflected by increased rates of prolonged hospitalilzation. Notably, those with ≥ 1 risk factor, and presumably those with DS and major CHD, faced the highest risk, with increased likelihood of PICU admission. As RSV prophylaxis becomes more widely adopted and potentially more affordable for infants under one year, additional and larger high-risk groups that may benefit from immunoprophylaxis will be more noticeble. Our results alone cannot guide policy, they provide supportive evidence for considering these groups in extended prophylaxis programs, pending confirmation from larger studies.

Comments (0)