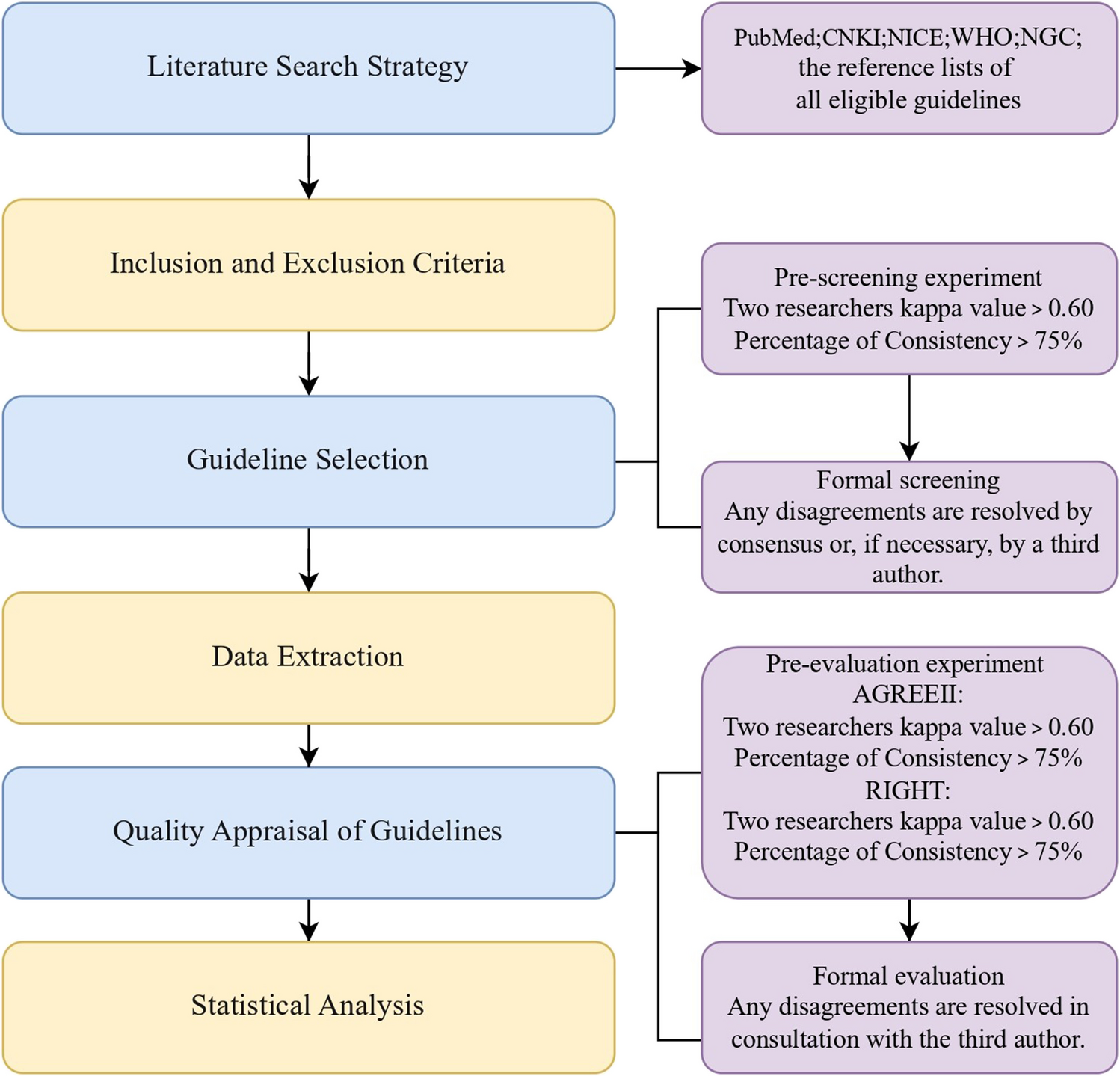
The findings of this study offer critical insights into off-label prescribing practices in pediatric care across Italian hospitals, shedding light on institutional disparities, regulatory compliance, and the impact of compassionate use programs.
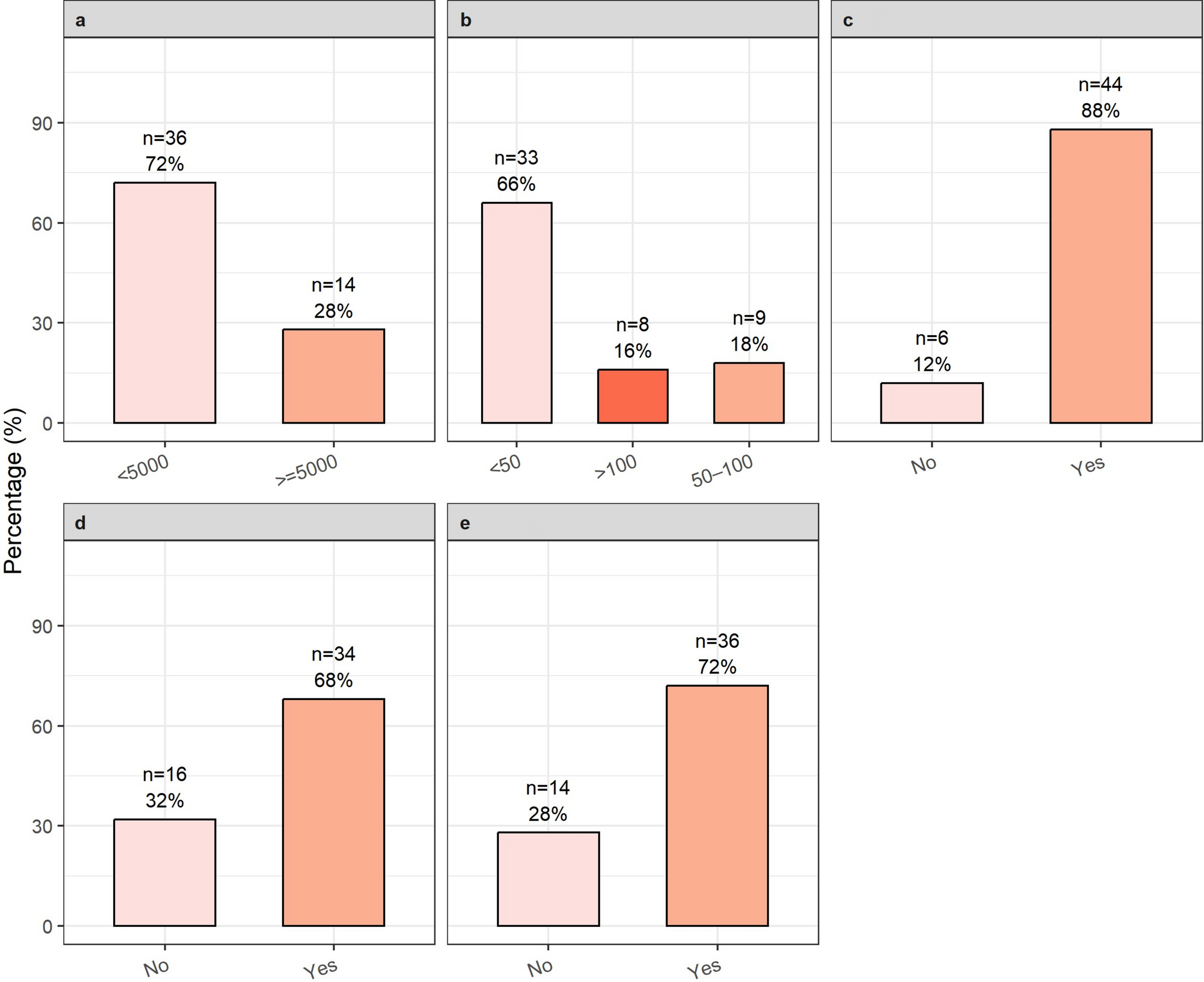
The surveyed hospitals displayed considerable variation in their infrastructure and resources. Despite the fact that 72% of facilities reported fewer than 5000 pediatric admissions per annum and 66% operated with fewer than 50 pediatric beds, a high proportion of these facilities (i.e., 64%) were equipped with both neonatal care units (NICU/NSCU) and birth centers.
Following the refusal of a compassionate use authorization, an analysis of off-label prescribing showed a strong association with NICU settings; the investigation indicated an augmented probability of off-label prescriptions, with a documented increase in the frequency reaching up to 50%. This finding is consistent with the results of previous studies that analyzed off-label prescriptions on a global scale. These reviews evidenced that, in the context of patients admitted to NICU wards, the proportion of subjects receiving at least one off-label or unlicensed drug prescription is notably higher than in patients on general medical and surgical pediatric wards [7, 49]. Therefore, a hypothesis can be formulated that suggests the practice of off-label prescribing is not solely dictated by the size of the hospital, but rather by the existence of specialized units dedicated to the care of pediatric patients.
Of the centers with more than 5000 admissions per year, 50% administer 100–500 off-label medications. It is a matter of concern that approximately 25% of all centers issuing prescriptions for off-labels were not aware of the frequency of prescriptions, highlighting significant deficiencies in documentation and monitoring procedures. The primary motivation for the prescription of off-labels is the pressing need for pediatric-specific drug formulations, as these combine therapeutic indication with age. This necessity is driven by the dearth of medications that have been expressly authorized for utilization in pediatric populations, a situation that is further compounded by the pressing need for therapeutic interventions for conditions that remain unaddressed by the existing range of approved treatments. This finding is consistent with the therapeutic areas where off-label prescriptions are predominantly utilized, such as neonatology and oncology.
The Pharmacy Unit was identified as the primary entity responsible for overseeing off-label prescriptions in 70% of the surveyed hospitals. However, one facility, with a prescription rate of more than 500 off-labels per year, indicated that off-label prescribing is managed directly within the clinical unit without the use of any operating procedure or managing system, raising concerns over adherence to regulatory safeguards. Furthermore, the facility in question has indicated that compassionate use requests are not submitted, and that no off-label cost-monitoring mechanism is in place.
It is noteworthy that paper-based record-keeping remains the predominant monitoring system, particularly in hospitals with lower off-label prescription rates. Conversely, institutions that have delegated the oversight of off-label prescriptions to a CTRU or an off-label evaluation committee utilize exclusively digital management systems. This suggests that technology may play a pivotal role in enhancing tracking and compliance mechanisms in structured facilities.
The findings demonstrate a substantial relationship between the availability of compassionate use and the prescribing trends of off-labels. The absence of compassionate use access has been demonstrated to significantly decrease the likelihood of off-label prescriptions, thereby underscoring the influence of regulatory barriers on the behavior of healthcare professionals. Institutions equipped with a CTRU exhibited a higher probability of receiving positive responses for compassionate use requests, thus reinforcing the role of dedicated research units in navigating regulatory pathways effectively.
Furthermore, monitoring off-label related costs has also been demonstrated to facilitate access to compassionate use. Indeed, centers that have established cost-tracking mechanisms have been found to be significantly more likely to receive positive responses for compassionate use requests. This association underscores the significance of financial oversight in regulatory approval processes, thereby ensuring that off-label prescriptions are aligned with the available institutional resources.
It is important to acknowledge that the question regarding access to compassionate use (i.e., “What is the positive response rate of pharmaceutical companies to compassionate use requests submitted by your organization?”) is poorly formulated, as it implicitly assumes that such requests are routinely granted. The observed strong correlation between off-label cost monitoring and access to compassionate use may instead reflect that institutions engaged in financial oversight are more likely to identify situations where compassionate use is both clinically justified and economically feasible. Consequently, these institutions may submit a higher volume of requests. However, this interpretation remains speculative and warrants further investigation.
A salient finding is the demonstrated correlation between the existence of an operational off-label prescribing procedure and an enhancement in cost-tracking practices. Nevertheless, the discordance between policy and practice remains a matter of concern. Two institutions claimed to have formal operational procedures yet failed to implement them effectively, illustrating potential regulatory inefficiencies.
This study has several limitations. The survey design may have introduced reporting bias, limiting causal interpretations and affecting data accuracy due to variability in institutional self-reporting. With only 50 of the 176 (28%) of invited facilities participating, generalizability may be compromised, and selection bias toward more engaged centers is possible. Additionally, differences in respondents’ roles and training across institutions may have influenced how questions were interpreted. Despite these limitations, the study offers a valuable national snapshot of off-label prescribing practices in Italian pediatric hospitals and lays the groundwork for future longitudinal and audit-based research.
The analysis has highlighted an overall absence of robust operational frameworks. In light of these results, a series of operational recommendations is hereby proposed to improve the management of off-label prescriptions in pediatrics.
Healthcare facilities should adopt standardized and enforceable procedures, supported by regular updates and internal audits to ensure consistency and regulatory compliance. Digital systems for tracking prescriptions and costs can improve transparency and support access to compassionate use programs. Training programs for clinicians, pharmacists, and administrators are essential to align practice with legal and ethical standards. Periodic audits should assess appropriateness and documentation quality. Strengthening CTRUs, even in smaller centers, can enhance engagement with pharmaceutical companies and broaden access to innovative therapies. Finally, structured benefit-risk assessment models—potentially integrated with AI—can support informed and safer prescribing decisions [27, 30, 50].

Comments (0)