Changes in the sagittal spinopelvic profile in patients with multiple myeloma
Throughout this study, we tracked alterations in sagittal spinopelvic profile parameters during the course of MM, uniquely incorporating a longitudinal approach to capture changes over time. Our findings highlight the evolving characteristics of sagittal spinal alignment in MM and their significance for patient care. The key findings of our study are the connection between kyphotic progression and pain, the prevalence and consequences of VCFs, and the clinical implications for spinal surgical interventions.
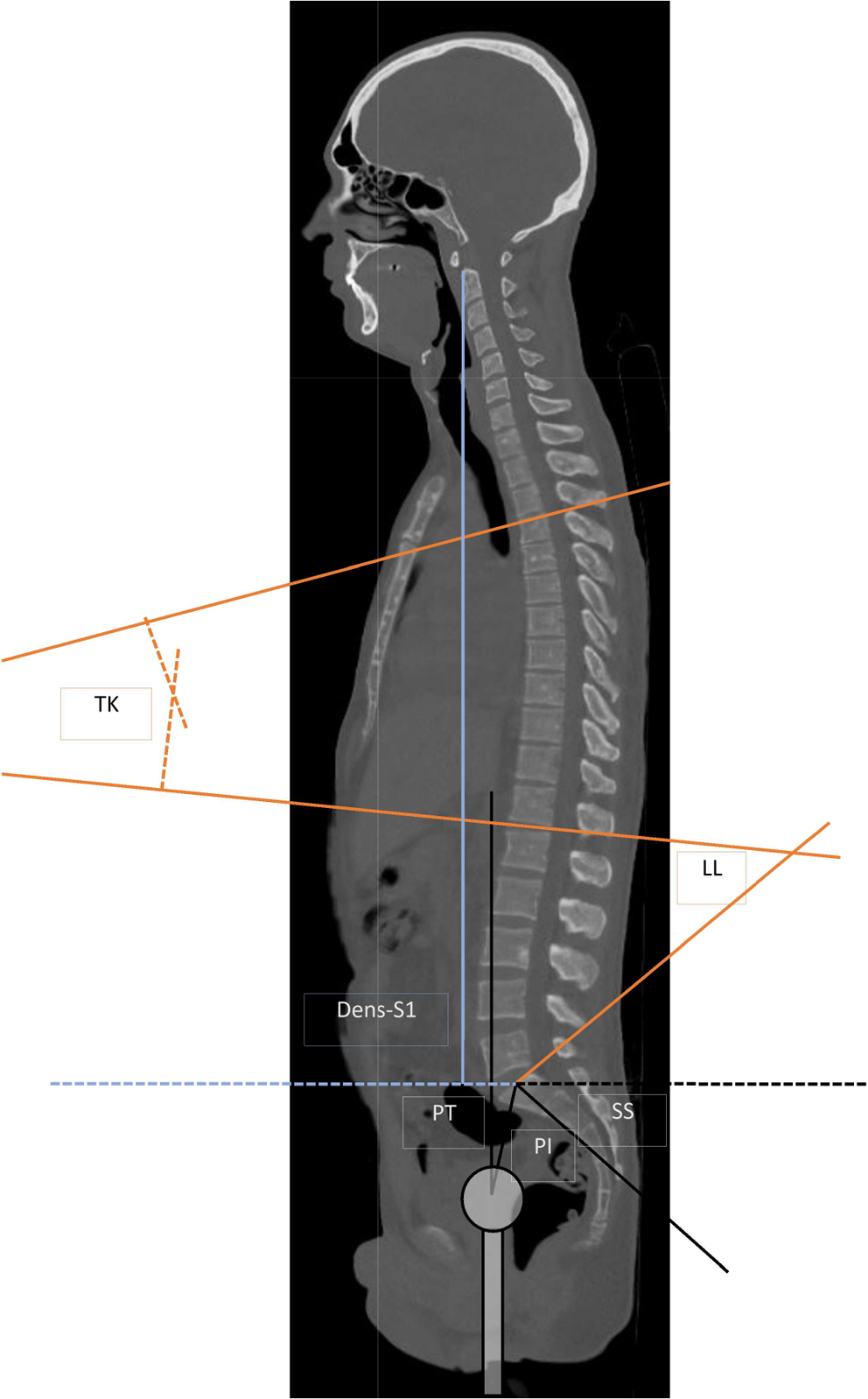
As the disease progressed, TK increased significantly, and the Dens-axis-S1 distance decreased, indicating a decrease in patient height. The data indicate a moderate effect size with a Cohen’s D of 0.55 for TK and a high effect size with a Cohen’s D of 1.55 for the distance from Dens to S1, which underscores the significance of these results. Although a 3.9 cm decrease in patient height may initially seem small, its clinical implications extend beyond mere anthropometric changes. First, this parameter serves as an indirect measure of cumulative structural impact on the spine, which is driven primarily by VCFs, bone loss, and kyphotic changes. Second, reductions in spinal height correlate with compromised pulmonary function due to restricted thoracic cavity expansion, which is particularly relevant in MM patients with preexisting frailty or comorbidities such as chronic obstructive pulmonary disease (COPD) or recurrent infections [16]. A reduced Dens-S1 distance, therefore, could contribute to a decline in overall physical function and an increased risk of pulmonary complications, which are known to be significant contributors to morbidity and mortality in MM.
These changes were accompanied by greater pain levels and greater analgesic use. In addition to TK progression and a reduced Dens-S1 distance, other factors likely contributed to the observed increase in back pain in this cohort. Senile osteoporosis and cancer-related bone destruction further compromise vertebral integrity and structural instability [17] due to the increased risk of VCF and periosteal nerve irritation [18]. Additionally, sarcopenia, commonly observed in MM patients, weakens the paraspinal musculature, reducing spinal support and increasing mechanical stress on the vertebral column [19]. Sagittal plane imbalance, as the spine compensates for kyphotic progression, further shifts the load-bearing axis anteriorly, leading to chronic pain and functional decline [20, 21]. Collectively, all of these factors, including TK kyphosis progression and a decrease in Dens-S1, create a multifactorial pathway that not only intensifies pain but also accelerates physical deterioration and diminishes overall quality of life.
Influence of vertebral fractures and spinal stabilization on patient outcomes
Our study also demonstrated that approximately 60% of patients experienced VCF over a three-year period. This finding is in line with earlier studies revealing an incidence of VCF ranging from 60 to 73% [22, 23]. Additionally, the presence of VCFs did not significantly increase pain levels or analgesic consumption. This contradicts findings from previous studies that correlated increasing numbers of VCFs with increased pain levels and deficits in functional status in MM [7, 24]. Our study, however, shifts the focus to a different perspective. Our data show that despite the direct effect of VCFs, an increase in TK itself might exacerbate pain. Changes in spinopelvic sagittal alignment, particularly with increased TK, prompt the posterior spinal muscles to intensify efforts to counteract kyphosis [25]. This exertion can result in muscle fatigue and a more pronounced kyphotic posture, potentially amplifying pain levels [26]. Patients may compensate for increased TK by retroverting the pelvis and augmenting LL [27]. Although we did observe increased TK with increased pain levels, we could not observe significant alterations in LL, PI, PT, or SS among the patient cohort. This observation may stem from the limited muscular coping capacity typically observed in elderly MM patients. The high prevalence of VCFs (60%) and the proportion of patients who underwent spinal stabilization (40%) are important factors that could have influenced our findings, particularly regarding the association between kyphotic progression and pain intensity in our patient cohort. The cumulative burden of multiple VCFs may play a role in worsening sagittal alignment over time, further stressing the paraspinal musculature and leading to progressive kyphotic deformity. The fact that pain levels increase with worsening TK but that analgesic consumption remains unchanged suggests that patients may experience worsening pain due to mechanical stress, muscular fatigue, and compensatory mechanisms related to spinal deformity rather than acute nociceptive pain directly linked to fractures [28, 29]. This finding is further supported by our finding that the presence of VCFs alone did not significantly correlate with increased pain or analgesic consumption. If alignment correction is inadequate, persistent sagittal imbalance may continue to place excessive strain on the spine, negating the expected pain-relieving effects of stabilization. These results indicate that while fractures and instrumentation are key variables in changes in spinal alignment, pain and function, kyphosis progression itself might also influence patient outcomes.
In line with this, our findings indicate that patients with a TK increase of less than nine degrees did not experience a significant rise in pain levels. However, when TK progression exceeded nine degrees, pain levels increased markedly. We defined TK progression cutoffs of < 5°, 5–9°, and > 9° for subgroup analysis on the basis of observed patterns in the general population. The Wakayama Spine Study demonstrated that the TK increases approximately 5° between age groups < 50 years to 60–69 years and another 5° between 60 and 69 years and 70–79 years. This progressive increase in TK correlated with worsening physical performance in the general population [30]. Given this association, we hypothesized that similar increases in TK in MM patients, such as pain (VAS) and analgesic consumption (WHO levels), might have a significant effect on clinical outcomes. Our data indicate that patients may effectively compensate for a TK increase of less than nine degrees, but further increases in TK exacerbate pain. Interestingly, these increased pain levels were not accompanied by increases in analgesic consumption in this subgroup. The absence of a difference in analgesic consumption despite higher pain levels may be explained by patient adaptation, opioid tolerance, or reluctance to escalate analgesic therapy owing to side effects [31]. Previous research revealed that patients with chronic back pain often endure worsening symptoms without increasing medication use, either because of the ineffectiveness of higher doses, physician-prescribed limitations, or personal reluctance to escalate opioid intake [31]. Additionally, patients may develop compensatory mechanisms to tolerate increasing spinal deformity, resulting in stable analgesic usage despite worsening pain.
Functional implications and clinical considerations
To further analyze our study population clinically, we monitored changes in the ECOG and ASIA scores. Even though patients with increased TK and decreased Dens-Axis-S1 distance experience increased levels of pain and analgesic consumption, the ASIA and ECOG classifications did not significantly decrease. The disparity between worsening kyphosis/pain and stable functional scores suggests that spinal deformities and pain might impact quality of life but not necessarily lead to further neurological deficits or broad functional decline.
Strengths and limitations of the study
This study has several limitations. Spinopelvic parameters were assessed using supine CT scans, which provide precise anatomical detail but may not fully reflect the functional spinal alignment observed in standing radiographs [32]. PT, LL, and TK decrease in the supine position, whereas SS increases, whereas PI remains unchanged [33, 34]. Standardized methods were applied to reduce measurement variability, but intraobserver reliability was not formally assessed.
Data collection was retrospective, relying on CT scans and patient records, which may not capture all clinically relevant factors. The effects of chemotherapy regimens, bisphosphonates, and systemic treatments on bone metabolism, muscle mass, and spinal stability have not been systematically analyzed [35, 36]. Among the 141 patients identified, only 86 met the inclusion criteria, with exclusions due to missing or low-quality imaging data, potentially introducing selection bias. While age and sex distributions were comparable between the included and excluded patients, direct comparisons of disease progression, spinal parameters, and functional outcomes were not feasible due to incomplete datasets.
The strengths of our study include its substantial sample size and long follow-up period of approximately three years. Additionally, this is the first study to examine specific spinopelvic parameter alterations and their influence on pain and functionality throughout the course of MM disease.



Comments (0)