Despite many advancements, such as a multidisciplinary approach, in the care of SD challenges continues to be challenging. To the present date there are no widely accepted standardized SD treatment pathways across different healthcare systems. Reliable real-life data on treatment pathways for SD can aid decision making algorithms and help in formulating realistic care expectations and quality reference data.
Readmission rates in spine surgery differ based on to their underlaying pathology. Following elective lumbar spine surgery a 90-day-all-cause readmission rate of 2.3% has been reported, whereas for metastatic spine surgery and fractures of the thoracolumbar region rates of up to 21.9% and 13.3% respectively were observed [19,20,21]. The data for SD readmission outcomes is far more limited. Previous small cohort studies published rates of 34.9% for SD and 37.1% for patients with spinal epidural abscess formations [15, 22]. Compared to other pathologies of the spine this rate is notably higher. The results of our study support these previously reported readmission rates derived from smaller studies surprisingly closely. Overall, we identified a 90-day-all-cause readmission rate for spondylodiscitis of 35%. The mean time to first readmission was 35.75 days (± 22.99). This timeframe is generally comparable to other spine pathologies [23]. Overall, a high rate of readmission in a relatively short time underscores the severity of this infectious disease, challenges in source control and treatments.
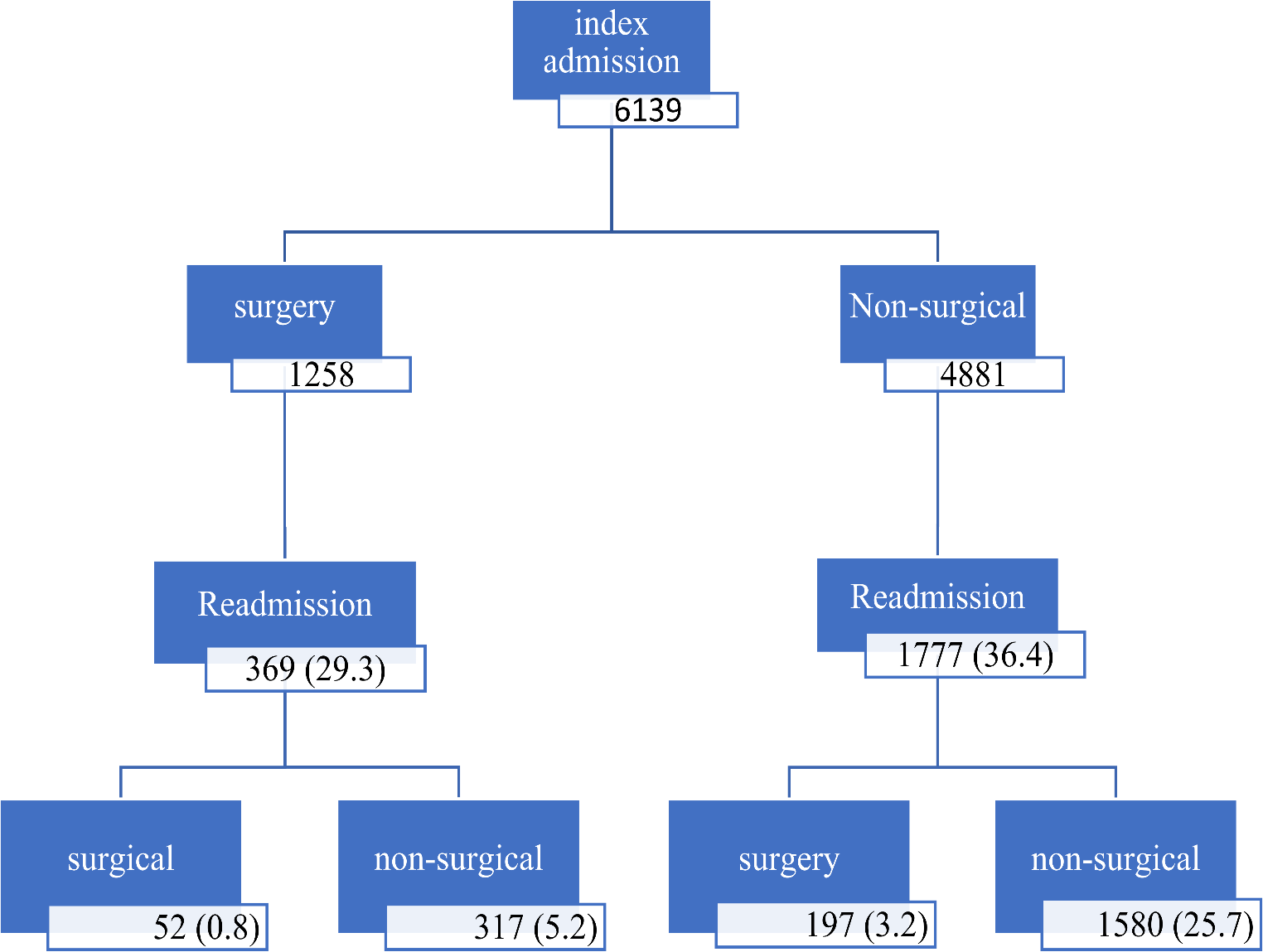
Our study revealed that the majority of patients were selected for an non-surgical management pathway upon index admission. Again our findings are consistent with previous more limited studies [9, 24]. Typically accepted indications for SD surgery are present or progressive neurological deficits, progressive spinal deformity or instability and inadequate response to medical treatment. Up to this date there is no consensus on timing of surgery, aside from emergency decompression for acute major neurological deficits. Due to advancements in surgical techniques and greater confidence based on evolving scientific knowledge it appears that early spine surgery might be more favorable for some patients [9, 24,25,26]. Additionally, early surgical interventions in combination with timely antibiotic treatment has shown to produce better functional outcomes and a shorter length of stay compared to standard medical treatment [8, 10, 25, 27]. However, indications for surgery are not accounted for in this current study. Our study revealed surgery on initial admission as an actually protective factor against readmissions. Patients treated surgically were significantly less frequently readmitted (29.3% vs. 36.41%) and the time until readmission for surgical patients was longer (surgical 41.65 days (± 22.84) vs. non-surgical 34.52 days (± 22.83). Not surprisingly, length of stay for surgical patients was significantly longer. As previously discussed the rate of readmission remains much higher compared to other spine pathologies, regardless of the treatment pathway. Nonetheless, our results, similar to previous research, do support some benefits of surgical care over non-surgical care. Our findings suggest that surgical treatment for SD may have a protective effect against readmissions by being more effective, reflected by fewer patients being readmitted later in time. This hypothesis is supported by previous publications which showed that early surgical treatment significantly outperformed non-surgical management in both failure and mortality rates, as well as LOS [10, 25]. Most recently, Neuhoff et al. reported a mortality rate of 24.2% for a non-surgical vs. 4.2% for a surgical group ( p < 0.001), with a LOS of 45.6 vs. 29.2 days respectively. Although the mortality rate in our study was much lower, the surgery group also demonstrated a lower mortality rate compared to the non-surgical group. The much lower LOS in our study, combined with the puzzling finding that the surgery group had a longer LOS than the non-surgical group, may be elucidated due to differences in healthcare systems as Neuhoff et al. study used European data.
Another interesting finding was that a non-elective admission status was identified as an independent risk factor for readmission. Although a non-elective admission status was common in both groups, non-surgical patients were significantly more commonly represented. This unexpected finding may appear perplexing at first. However, previous study have found that delayed diagnosis or initiation of treatment adversely affects patient outcome and increase mortality [8, 25, 27]. Elective admissions may represent a delayed initiation of treatment, resulting in the found increased odds for readmission. Furthermore delays, caused by an scheduled elective admission, may result in progression of the disease to a more severe state by the time of treatment. The finding that a fewer surgical patients were admitted non-electively than non-surgical patients may be due to cases in which surgical treatment was indicated but not immediately.
Our analysis showed a significant difference in time to readmission for the different treatment pathways following readmission. Out of all patients readmitted surgical revisions were the least common, accounting for 0.8% of all patients, with longest time to readmission (50.85 (± 24.27). Conversely the majority of patients (25.7%) readmitted received non-surgical treatment with the shortest time to readmission (34.16 (± 22.64). A transition from surgical to non-surgical treatment was required in 5.2% and 3.2% of patients respectively. Prior publications on conversion of treatment pathways are limited with an incidence from 13% up to 28.5% reported, without much further evidence published [14, 26].
These high rates may be attributed to disease progression, which can lead to complications such as mechanical instability or epidural abscesses, warranting surgical intervention.
As previously mentioned appropriate surgery in combination with antibiotic therapy resulted in better patients’ outcome overall [24, 26, 27]. Although our transition rate was much lower the findings of this study suggest that patients benefited from primary surgical SD treatment. Potentially expanding targeted indications for surgical treatment in SD might be a reasonable consideration for instance by applying a validated risk-based scoring system [11].
This study has several without limitations. The retrospective design and reliance of administrative date gathered by the Healthcare Cost and Utilization Project (HCUP) inherently introduce bias and limit the availably of to generalize findings. The global COVID-19 pandemic, affecting clinical practices in a multi-factorial fashion, may have influenced data. Patient comorbidities and psychosocial considerations as well as resource restrictions may have influenced initial decision making in selecting patients for non-surgical and surgical care. Further research could aim to delve into benefits of using a standardized decision-making algorithm in management of SD. Furthermore research into expanding indications for surgical treatment in SD may be beneficiary.



Comments (0)