
Remember me
We used data from the cross-sectional MRI substudy within the “Cooperative Health Research in the Region of Augsburg” (KORA) cohorts [16]. The MRI examination was done within the second follow-up KORA-FF4 (N = 2279, enrolled in 2013/2014) of the original population-based KORA-S4 survey (N = 4261, enrolled in 1999/2001). Of the KORA-FF4 cohort, N = 400 participants underwent whole-body MRI within 33 days (interquartile range: 24–45 days) of their examination at the study center. Inclusion criteria were no contraindications to MRI (claustrophobia, allergy to contrast agent, permanent metal parts in the body), age < 74 years, being in generally good health sufficient for the one-hour whole-body imaging procedure, and no prevalent cardiovascular disease (stroke, myocardial infarction, revascularization) [16]. Additionally, N = 1010 participants of the KORA-FF4 cohort in the age range 48–68 years underwent pulmonary function testing [17]. The overlap of these two samples constitutes the analytical sample for the current analysis. The Ethics committee of the Bavarian Chamber of Physicians approved the general KORA cohort studies. The Ethics Committee of the Ludwig-Maximilians University Munich (Munich, Germany) additionally approved the whole-body MRI substudy (No. 498 − 12). The study was carried out in accordance with the Declaration of Helsinki and obtained written informed consent from all participants. Clinical trial number: not applicable.
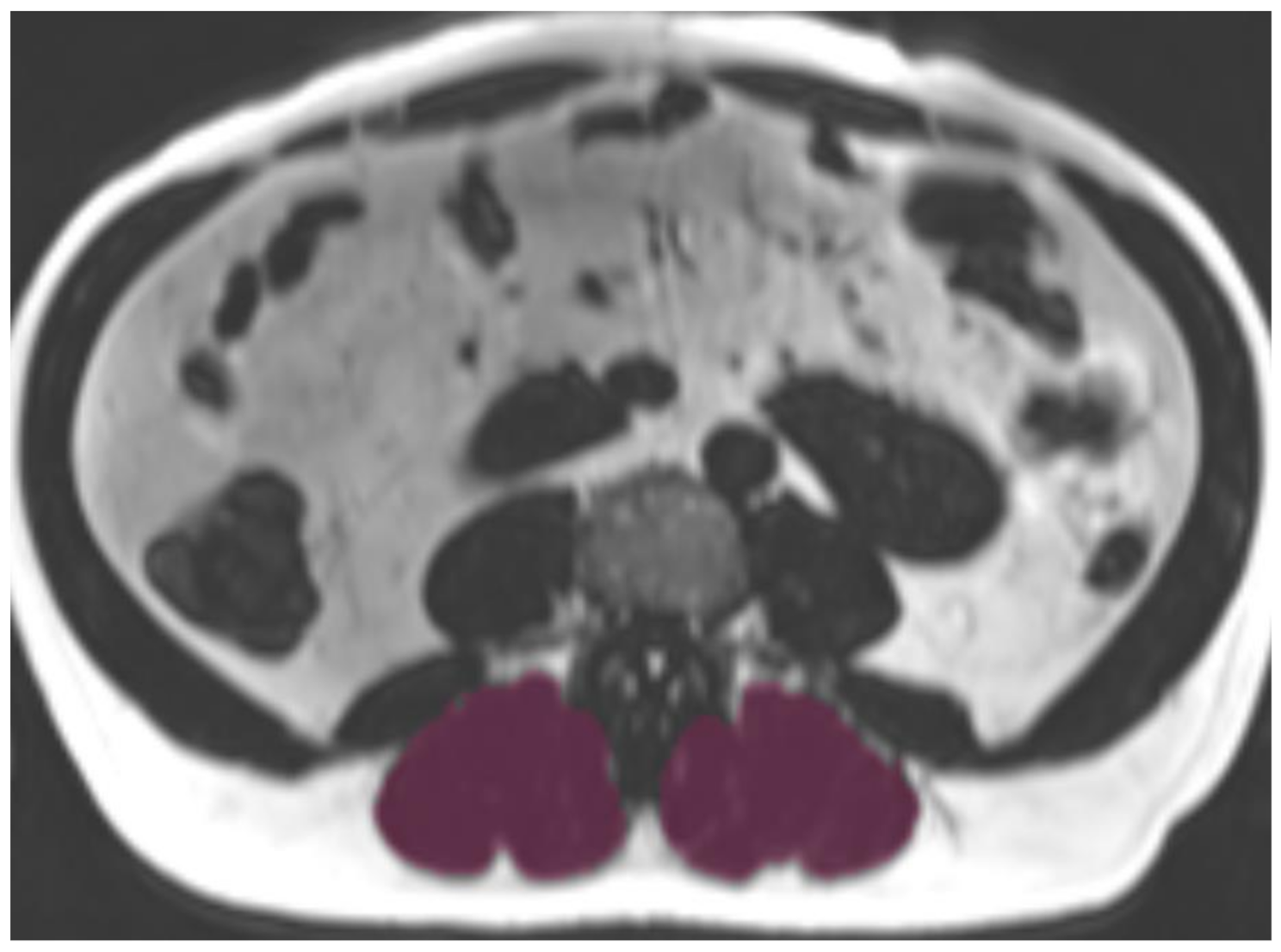
MRI protocol and muscle segmentationMRI examinations were performed using a 3 Tesla Magnetom Skyra scanner (Siemens Healthineers, Erlangen, Germany) with combined 18-channel body surface and spine matrix coils. The complete imaging protocol and technical specificities have been described in detail previously [16]. For muscle analysis, T2*-corrected multi-echo 3D-gradient-echo Dixon sequences of the upper abdomen were acquired during a single breath-hold (slice thickness 4 mm, voxel size 1.8 × 1.8 mm, field-of-view 393 × 450 mm, matrix 256 × 179, TR 8.90ms, TEs 1.23, 2.46, 3.69, 4.92, 6.15, 7.38ms, flip angle 4°). Accurate transverse slice positioning at L3 vertebral level was confirmed using coronal two-point Dixon gradient-echo sequences (TR 4.06ms, TE 1.26 and 2.49ms, flip angle 9°, slice thickness 1.7 mm, isotropic in-plane resolution 1.7 mm) with cross-reference. Paraspinal muscles were manually segmented at the level of the third lumbar vertebra by two observers blinded to clinical data and COPD status using standardized anatomical landmarks (MITK V2015.5.2, German Cancer Research Center, Heidelberg, Germany). Skeletal muscle area (mm2) was defined as the sum of the left and right areas of the paraspinal muscles (Fig. 1).
Fig. 1
Representative axial T2*-corrected multi-echo Dixon MRI slice (fat contrast) at level L3 with superimposed paraspinal muscle segmentation (purple). Manual segmentation was performed bilaterally using standardized anatomical landmarks
Abbreviations: MRI: magnetic resonance imaging; L3: 3rd lumbar vertebra
Myosteatosis quantificationTotal myosteatosis was determined as proton density fat fraction (PDFF, in %). PDFF maps were calculated from the original data using the manufacturer’s software (MR Liverlab, Version VD13, Siemens Healthineers, Cary, USA). Mean PDFF was calculated by averaging measurements from right and left muscle compartments, including IMCL, intramuscular and subfascial intermuscular EMCL, while excluding surrounding extrafascial intermuscular EMCL. The reproducibility of this segmentation approach was previously validated in a methodological study using the same protocol, demonstrating excellent reliability with intraclass correlation coefficients of 0.98 and 0.99 for inter- and intra-observer agreement of PDFF measurements, and 0.97 and 0.98 for muscle area measurements [18].
For differentiation of fat compartments, IMCL were quantified by postprocessing the segmented muscle compartments using a semi-automated algorithm (Matlab_R2017a; MathWorks, MA, USA). This algorithm applies an established threshold based on the understanding that myocytes with high intramyocellular lipid content demonstrate values ≤ 20%, while higher values indicate the presence of extramyocellular adipose tissue [12]. This 20% PDFF threshold follows the physiological rationale, where values below 20% reflect small intracellular lipid droplets and above 20% larger adipocyte aggregates [19]. Accordingly, voxels with PDFF values ≤ 20% were classified as containing IMCL, while EMCL content was calculated as the difference between total paraspinal myosteatosis and IMCL, comprising predominantly extramyocellular intramuscular fatty septa and subfascial intermuscular adipose tissue [18].
Pulmonary function testingAs reported previously [20], three categories of pulmonary function indices were analyzed: (1) Spirometric indices including forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1/FVC, and forced expiratory flow between 25% and 75% of FVC (FEF25–75); (2) lung volumes derived from single-breath measurement of pulmonary gas exchange, which include residual volume (RV), functional residual capacity (FRC), total lung capacity (TLC), and alveolar volume (VA); (3) indices of pulmonary gas exchange, which include transfer factor of the lung for carbon monoxide (TLCO) and the transfer coefficient TLCO/VA. Standard spirometry without bronchodilation and single-breath measurement of TLCO were performed in line with German as well as American Thoracic Society (ATS)/European Respiratory Society (ERS) recommendations in upright sitting position using a pneumotachograph-type spirometer (MasterScope PC and MasterScreeen PFT, CareFusion, Höchberg, Germany) [21]. At least three and up to eight spirometric maneuvers and up to five single-breath TLCO maneuvers were performed to obtain a minimum of two acceptable and reproducible measurements. COPD was defined as FEV1/FVC below the Lower Limit of Normal (LLN) based on American Thoracic Society and European Respiratory Society recommendations using Global Lung Initiative reference values that are based on age, sex, height and ethnicity [22, 23].
Clinical covariatesAll participants underwent standardized interviews and physical examinations at the study center. Anthropometric measurements, including weight, height, and body mass index (BMI), were obtained according to standardized protocols. Blood pressure measurements were performed to assess hypertension, defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or current antihypertensive medication. Laboratory analysis of fasting blood samples included the determination of blood lipid parameters (HDL, LDL, and triglycerides) and inflammatory markers (hsCRP) by standard laboratory measures. Smoking behavior was assessed by self-report and classified into never, former and current smoker. Study participants were classified as physically active (regular physical activity ≥ 2 h/week or approximately 1 h/week) or physically inactive (irregular physical activity < 1 h/week, almost no or no physical activity), based on self-report.
Statistical methodsParticipants’ baseline characteristics for the whole sample and stratified by COPD status are presented as mean and standard deviation or median with interquartile range for continuous data, and counts and percentages for categorical data. Differences between groups were quantified by t-test or Wilcoxon-test, and χ2 test or Fisher’s exact test for groups with n < 5, respectively.
Univariate correlations between MRI-derived skeletal muscle parameters and pulmonary function were quantified by Spearman’s correlation coefficient.
To evaluate the association between MRI-derived skeletal muscle parameters as exposure and pulmonary function parameters as an outcome, adjusted linear and logistic regression models were applied. Models were adjusted for 1) age and sex, 2) age, sex, smoking, diabetes, physical activity (yes/no), and BMI, and 3) Model 2 plus hsCRP. All exposures and continuous outcomes were centered and scaled (minus mean and divided by standard deviation) before modelling. Results are given as beta coefficients or Odds Ratios (OR) with respective 95% confidence intervals.
R version 4.4.1 was used for statistical analysis. P-values < 0.05 were considered to denote statistical significance of associations, without adjustment for multiple testing.
Comments (0)