
Remember me
A total of 31 male adults enrolled in the study with 22 participants completing all aspects of the protocol. Please refer to Fig. 1A for demographic information. Participants self-reported normal or corrected-to-normal vision; normal hearing; no history of psychological, neurological, or other medical diagnoses; no use of tobacco in the past six months; and no excessive alcohol use. Thirteen participants reported previously experiencing hypoxia. The study protocol was approved by the Naval Medical Research Unit– Dayton’s (NAMRU-D) Institutional Review Board (NAMRUD.2022.0003) in accordance with the principles embodied in the Declaration of Helsinki and local statutory requirements and all participants provided written informed consent prior to participation.
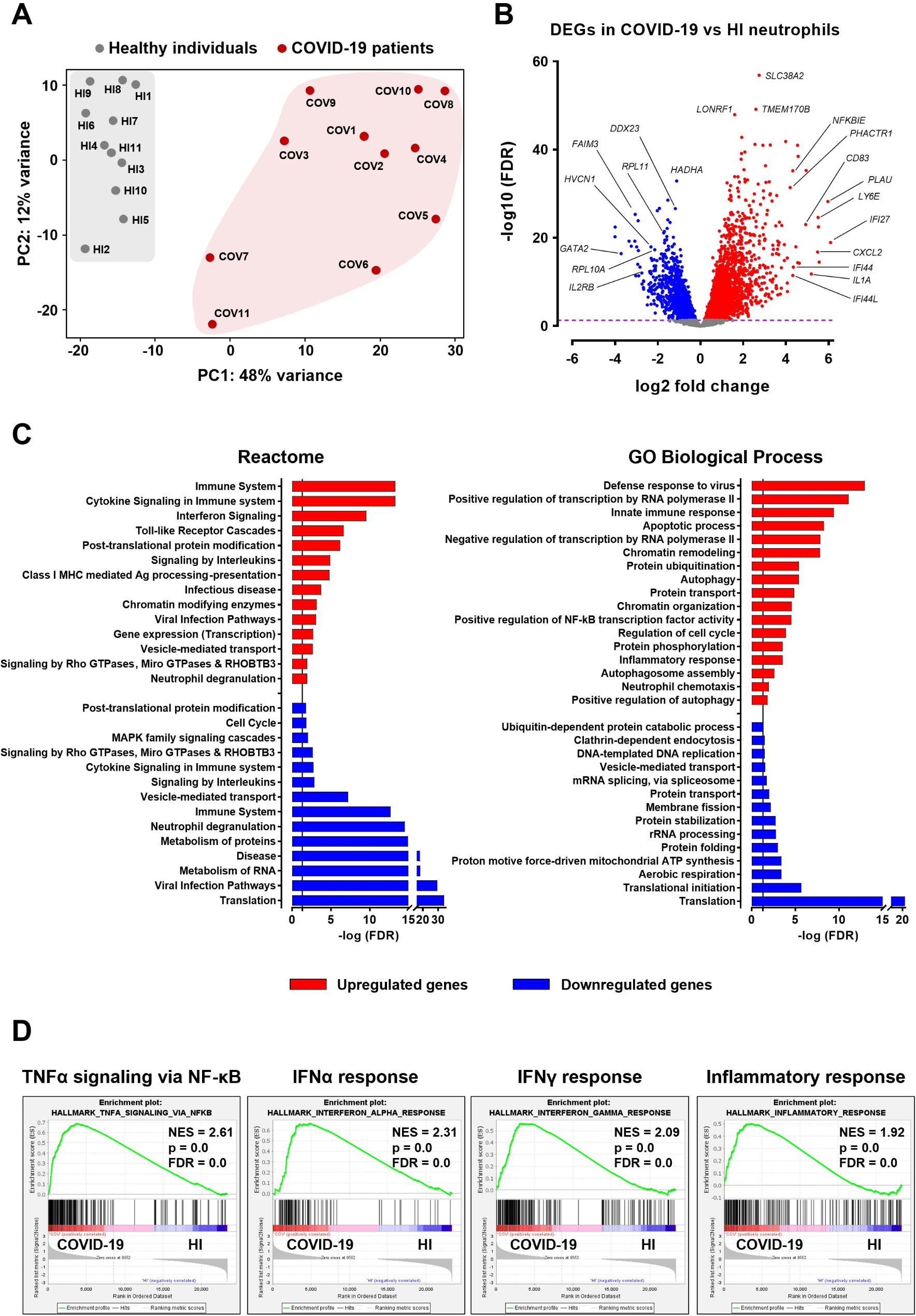
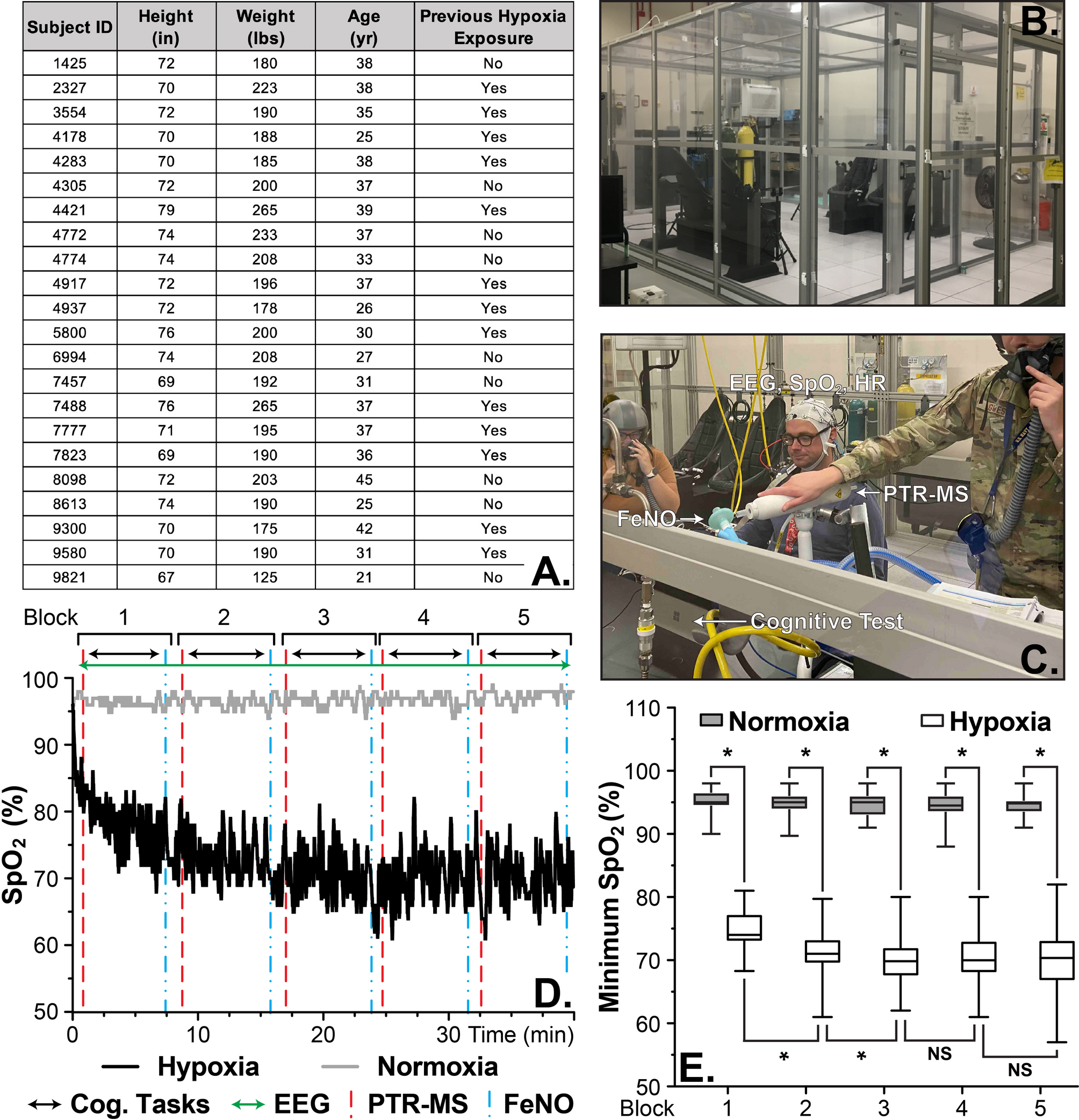
Fig. 1
Experimental setup and measured oxygen saturation for each exposure, normoxia and hypoxia. (A) A summary of the available demographic data. (B) An image of the Reduced Oxygen Breathing Environment (ROBE) used for the two exposures. (C) An image of the experimental setup within the ROBE. (D) A figure depicting both the sampling times and a representative SpO2 trace from normoxic and hypoxic exposures. (E) A box plot of the minimum SpO2 from the exposures by sampling block. * indicate p < 0.05, NS = not significant, and error bars represent the min/max values. The results show a significant reduction in oxygen saturation (SpO2) in the hypoxic condition compared to the normoxic exposure
Hypoxia & normoxia exposuresThe exposures were single-blinded, with participants performing three visits on separate days. The initial visit, participants provided written informed consent and demographic information; completed screenings for eligibility; and conducted a familiarization session for each cognitive task. Approximately one week following the initial visit, participants completed two experimental visits at approximately the same start time in counterbalanced order of exposure condition, altitude oxygen (hypoxia) and sea level oxygen (normoxia), with at least 36 h between the experimental visits (µ = 4.7 ± 5.90 days).
Each 45-minute exposure was conducted in a ROBE (Fig. 1B), a normobaric hypoxia chamber, with the ROBE held at approximately 10.6% O2 (17,500ft equivalent) for the hypoxic condition and 21% O2 for the normoxic condition. Please refer to Supplemental Data 1 for a representative example and a box plot of the measured O2 of the ROBE during the exposures. Prior to entering the ROBE, an EEG cap was donned, a fractional exhaled nitric oxide (FeNO) sample was collected, and participants provided blood samples. Upon entering the ROBE, participants immediately began tasks, which consisted of five, 8-minute testing blocks where participants provided two breath samples within the PTR-MS, performed six minutes of randomized cognitive tasks, and provided a FeNO sample (Fig. 1C and D). Please refer to future sections for details of each task within the ROBE. Upon completion of the exposure, participants were provided 21% O2 through a Hans Rudolph oronasal mask until their peripheral oxygen saturation (SpO2) was ≥ 90%. Participants exited the ROBE, completed a hypoxia symptom questionnaire (HSQ), and provided an additional FeNO sample as well as a blood sample and an oral/salivary sample. Of note, while the blood (global metabolomics) and salivary samples were collected within this study, they will not be discussed here.
Physiological measurementsThroughout both exposures, participants’ SpO2 and heart rate (HR) were monitored and recorded at 1 Hz. Both measures were acquired via a finger-mounted pulse oximeter and recorded by an Apple iPad via Bluetooth connection (Nonin Medical Inc., Plymouth, MN, USA). Please refer to Fig. 1D and E and Supplemental Data 2 for representative measured SpO2 and HR data along with summary data for all participants. The three lowest SpO2 (minSpO2) values within a block were averaged and used for further analysis. A safety cut-off criterion of 60% SpO2 for all participants was used, whereby an individual was provided supplemental oxygen and their exposure prematurely ended upon exceeding this limit.
PhlebotomyApproximately, 16mL total of unfasted whole blood was drawn from each volunteer’s arm (4mL into each K2 EDTA (purple top), Lithium Heparin (green top), CAT serum (red top), and PAXgene RNA tubes (BD Biosciences, Franklin Lakes, NJ, USA, & Greiner Bio-One Monroe, NC, USA). The collection area was cleansed with a 70% alcohol swab and wiped with sterile gauze (BD Biosciences). A Greiner Bio-one 21G x 1” multi drawing needle with hub was inserted into the vein and tubes were inserted onto the needle assembly until full. The needle assembly was removed, and sterile gauze was placed over the site. Each sample type was prepared as instructed by the manufacturer, aliquoted, and stored at -80 °C until analyzed.
iSTAT blood chemistry & gasesBlood chemistry and gases were evaluated using an i-STAT point of care device affixed with an i-STAT CG8 + cartridge which measures sodium; potassium; ionized calcium; glucose; hematocrit; hemoglobin; pH; partial pressure of carbon dioxide (PCO2); partial pressure of oxygen (PO2); total carbon dioxide (TCO2); bicarbonate (HCO3); base excess (BE); and oxygen saturation (sO2) (Abbott Laboratories, Abbott Park, IL, USA). Briefly, the iSTAT instrument was evaluated for quality control and the CG8 + cartridge was warmed to room temperature. A small portion (~ 100µL) of sample was removed from a thoroughly mixed lithium heparin (green top) blood tube within 10 min of sampling and added to the device. Data was recorded and tabulated manually.
Hypoxia symptom questionnaire (HSQ)A 15-item hypoxia symptom questionnaire (HSQ) was utilized to measure each participants’ symptomology following each exposure on a 4-point scale (0 = not observed, 3 = severe) [22]. The HSQ was developed directly from the U.S. Navy’s hypoxia familiarization training program and contains items related to commonly experienced hypoxia symptoms.
Cognitive tasksParticipants were seated approximately 65 cm from a 13.5” tablet affixed with a standard keyboard modified to cover the symbols and reveal only the numbers (Fig. 1C, HP, Palo Alto, CA, USA, ). Each task, detailed below, was presented randomly for two-minutes within each six-minute block, on the tablet screen. All cognitive tasks were custom built in NetBeans and were run using Apache Ant 1.8.0.
Psychomotor vigilance taskThe Psychomotor Vigilance Task (PVT) is a simple visual reaction time (RT) test. Briefly, participants were presented with a red counter on a grey background which counted up from zero. Participants were instructed to strike any key on the keyboard once the number was observed. RT was the time, in milliseconds, from stimuli appearance on the screen to key striking. The stimuli remained on-screen for 1,000ms after a response was recorded to provide the participant with performance feedback. The interstimulus intervals were distributed randomly from 1,000ms to 5,000ms [23]. RTs were filtered, tabulated, and recorded.
Digit symbol substitution taskThe Digit Symbol Substitution Task (DSST) is a measure of associative declarative memory. First, participants were presented with a sequence of ten pairings of numbers and symbols on the keyboard (e.g., 1 and!, 2 and @, 3 and #, 4 and $, and so on). The first presentation of a number was paired with the corresponding symbol. Once all ten pairings had been introduced, only symbols (e.g.,!) were presented on-screen in a random fashion. Participants were instructed to press the number on the keyboard that corresponded with the presented symbol stimulus. Stimuli were presented in a random order for 5,000ms, with 1,000ms between stimulus presentations. Error in associations and response times were tabulated and recorded [24].
Change signal taskThe Change Signal Task (CST) measures an individual’s response to inhibition. Participants were initially presented with a “Go Signal” displayed on-screen (i.e., an arrow pointing left or right) and instructed to indicate the direction of the “Go Signal” by striking the corresponding arrow key on the keyboard. In 33% of trials, a “Change Signal” (a larger arrow) was presented after the “Go Signal”, indicating to participants to respond on the keyboard by striking the arrow key pointing in the opposite direction of the “Go Signal”. The time delay between the “Go Signal” and the “Change Signal” (stimulus onset asynchrony) fluctuated between 20ms and 800ms based on a staircase procedure, such that the initial delay was 200ms and decreased by 50ms when participants successfully changed responses and increased by 100ms when participants unsuccessfully changed response. Two error conditions were presented (low and high), which differed with respect to the color of the “Change Signal’s” arrow [25]. Error in “Change Signal” accuracy and reaction time were tabulated and recorded.
EEG: Event-Related potentials (ERP)The EEG data were recorded continuously from 32 electrodes in an elastic electrode cap uniformly covering the entire scalp, at 500 Hz with electrode impedance for all channels < 25kΩ and referenced to FCz in DC mode (LiveAmp, Brain Products GmbH, Gilching, Germany). Auditory tones were presented to the participant every 500ms at 85dB sound pressure level throughout the exposure within the ROBE via Etymotic ER3-A insert earphones (Lucid Hearing, Fort Worth, TX, USA). Participants were instructed to ignore the tones and to focus only on the tasks within the blocks. A passive auditory oddball paradigm was used that comprised a sequence of tones (n = 5,100). 85% of the tones were considered standard (50ms at 1,000 Hz) and 15% were deviants, either differing in duration (100ms at 1000 Hz) or both duration and frequency (i.e., “double-deviant”; 100ms at 1,100 Hz) [26,27,28,29,30]. All tones had a 5ms rise/fall.
The EEG data were processed using the Fieldtrip software package within the MATLAB operating environment [31]. The data were segmented into epochs covering the time from 100ms prior to and 500ms following the onset of each auditory stimulus presentation. The data were low-pass filtered at 20 Hz and referenced to the average of both mastoids (TP9, TP10). An independent components analysis (ICA) was performed and the eye blink and lateral eye movement components were removed. The EEG waveforms from frontal electrodes (i.e., Fp1, Fp2) were visually inspected for voltage fluctuations typical of gross motor movements (i.e., amplitude > ± 75µV) and trials containing these types of artifacts were rejected. The average waveforms were calculated for deviant and standard stimulus response within the six-minute cognitive task blocks throughout each exposure, using electrode Fz for analyses. Of note, one participant had excessive Fz noise and alternatively the Cz electrode was used. In this case, the nearest midline electrode to Fz was chosen based on visual inspection of topographic maps rather than a group of adjacent lateral electrodes. These data show the MMN/P3a complex was maximal over the frontal midline sites and similarly distributed between Fz and Cz [7].
The difference waves were calculated for each six-minute cognitive task block by subtracting the averaged standard response from the averaged deviant response. Additionally, the difference waves were calculated for the entire exposure to examine exposure changes. The mismatch negativity (MMN) was defined as the most negative-going difference waveform between 50ms and 300ms and the P3a was defined as the most positive-going difference waveform between 150ms and 400ms. To compromise between peak- and mean-based measures, the mean amplitude in a 100ms window, centered around the peak such that the window varies for each dataset, was reported [32]. The MMN/P3a mean amplitude and latency as well as peak-to-peak amplitude (P2P) were found separately for each six-minute block of each visit.
Proton transfer Reaction-Mass spectrometry (PTR-MS)Upon entering the ROBE, participants situated themselves at the table as depicted in Fig. 1C. Within two minutes of entering, each participant provided duplicate complete exhalations, both upper and lower/tidal breath, approximately 30s apart into the Buffered End-Tidal Breathing (BET) inlet affixed with a new non-rebreathing mouthpiece. Thirty seconds was found to be the approximate time that the breath signal within the instrument returned to baseline following an exhalation. Breath was sampled from the BET via a 70 °C heated line into an Ionicon Analytik Proton Transfer Reaction Time of Flight Mass Spectrometer 4000 sampling at approximately 50mL min-1 (PTR-MS, Innsbruck, Austria). All exhaled breath data were collected with H3O+ ionization utilizing the instrumental parameters described previously [33]. Briefly, spectra were acquired every 250ms over 5-389 m/z with a max flight time of 25µs and a 2µs extraction time. The source was operated with a drift temperature of 70 °C, a drift pressure of 2.8mbar, and a drift voltage of 680 V yielding an approximate E/N ratio of 124Td. The time of flight (TOF) detector was operated at approximately 4 × 10− 7 mbar. Every 20s during acquisition, the mass axis was automatically recalibrated using the H3O+ O18 isotope (21.02 m/z) and two PerMaSCal fragments (203.95 m/z and 330.85 m/z). The instrument was run continuously throughout the entire exposure. Daily checks of 100ppb isoprene dry compressed gas standard were used to verify instrument performance (≤ 10% RSD across all data collection days) and approximately 20 background spectra within the ROBE were collected prior to each exposure using the settings described above. Hydronium (21.02 m/z) was monitored throughout the experiment and a representative example trace is provided in Supplemental Data 3.
All spectra were manually evaluated within Ionicon Analytik’s PTR-MS Viewer Software, as described previously (v. 3.4.4) [33]. Briefly, a Gauss fit function and a 3-point mass calibration was applied to the imported.h5 data files using ions 21.02 m/z, 203.95 m/z, and 330.85 m/z. Exhalations were visualized using acetone (59.052 m/z) and isoprene (69.075 m/z) ions within the “Analyze Trace” feature of the PTR-MS Viewer software. The parts-per-billion (ppb) values of ten scans within each tidal portion of the exhalation were exported for 135 total ions (features). The exported feature concentrations were averaged for the two exhalations within each block. The data were filtered to remove features related to hydronium and water adducts, those above m/z 200, and those below the instrument limit of detection (LOD) based on three standard deviations (3σ) of the zero-air measurement for each feature within exhaled breath samples. The remaining feature list, of 89 features, was exported for further statistical analysis as described in a future section. Please see Supplemental Data 4 for feature quantities and LOD values.
Fractional exhaled nitric oxide (FeNO)Fractional exhaled nitric oxide (FeNO) was measured following the cognitive testing within all blocks as well as pre/post-exposure on an EcoMedics Analyzer CLD88sp affixed with a DENOX 88 nitric oxide (NO) free air supply (Fig. 1C, ECO MEDICS, Switzerland). Briefly, the instrument was NO zero- and flow-calibrated on every test day with a span calibration monthly, as per the manufacturer’s recommendation. The participants were instructed to breath normally and gently in and out of the mouthpiece for 45s while utilizing a nose clip. The instrument was operated in “multiple breath NO test” mode. All data were manually evaluated in the EcoMedics Spiroware software (v. 3.3.2) as recommended by the manufacturer. In short, the plateau borders from each breath within the multiple breath test were reset using the software’s default, 60–80% of the exhaled volume. In the event the reset caused the plateau borders to be located near a portion of the breath that had a significant slope, the boundaries were manually adjusted while staying within 40–90% of the exhaled volume. The average FeNO and the coefficient of variance (%CV) for each breath within a sample was determined, by the software, and evaluated. The minimum and maximum values from each overall sample were removed until a %CV of > 5% for < 4 breaths or > 10% for > 5 breaths was achieved. The data was exported and further filtered to remove any breath with a Plateau Average Flow (mL s-1) less than 200mL s-1.
Statistical analysisBasic figures and statistics were created in PrismGraphpad (v. 10.1.1). All data cleaning and statistical analyses were performed in the RStudio software suite (v.2022.12.0 + 353). All p-values for testing among breath conditions and background were computed using a Wilcoxon signed rank test due to small sample size and lack of normality in the data. Statistical significance was defined as p < 0.05. The significant features were used to predict the average SpO2 through linear mixed modeling with data reduction as shown below. Additionally, application of the reduced model to EEG and PVT data was conducted as illustrated below.
The full linear mixed model is represented below, where n is 13 features, epsilon (ε) is the random error, the breath features (BF) are the fixed effects, and the participant is the random effect to account for non-independence of the repeated time point of each participant. The full model was evaluated with relation to SpO2 as shown in (A) below. The model was reduced by bidirectional reduction, yielding a reduced model consisting of a k of 8 features and epsilon (ε) is the random error (B below).

The reduced model was applied to the 8 features (k) and epsilon (ε) representing the random error with relation to changes in EEG amplitude and PVT reaction time as shown in (C) and (D) above.
Comments (0)