
Remember me
A total of 234 patients with PC were included in this study. The most common immunosuppressive condition was caused by the use of corticosteroids and/or immunosuppressive or cytotoxic agents, while the most frequent comormidity was diabetes mellitus (14.5%) (Table 1).
Among them, 33 patients (14.1%) were classified into the SID group. The MID group included 69 patients (29.4%). The CO group comprised 17 patients (7.2%) who did not meet the criteria for MID nor SID. The remaining 115 patients (49.1%) had no identifiable underlying diseases or immunological abnormalities and were categorized as the IC group.
Epidemiological characteristicsAmong the 234 PC patients, 145 (61.9%) were male and 89 (38.1%) were female, resulting in a male-to-female ratio of 1.63:1. No significant difference was observed in sex distribution across the various immune status groups. The demographic characteristics of the cohort are summarized in Table 2. The average age of the patients was 50.66 ± 14.09 years, ranging from 18 to 88 years old. Notably, the IC group was significantly younger than the CO, MID, and SID groups (p < 0.05).
Table 2 Demographic characteristics of 234 patients with pulmonary cryptococcosis with different immune statusThe cohort was predominantly composed of patients residing in eastern Fujian Province (51.7%), followed by central Fujian (22.2%), southern Fujian (9.4%), northern Fujian (6.8%), and western Fujian (5.6%), suggesting a higher prevalence of PC in the southern subtropical climate region (Supplementary Table 1). No significant regional distribution differences were found between different immune status groups.
Most of the patients reported no prior environmental exposure to birds droppings within the 6 months prior to PC diagnosis. Among those with potential exposure, the most common factors included keeping or handling birds, especially pigeons, and/or direct contact with their droppings (9.4%). There were no significant differences in environmental exposures across the immune status groups.
Clinical featuresClinical symptoms and signsThe clinical symptoms and signs in relation to immune status are summarized in Table 3. The most common symptoms were cough (55.1%, 129 cases), sputum production (45.7%, 107 cases), chest pain (13.7%, 32 cases), and dyspnea (10.3%, 24 cases). Fever was less common, occurring in only 6.8% (16 cases) of patients. The incidence of dyspnea was significantly higher in the SID group compared to the MID group (p < 0.05). Fatigue was significantly more prevalent in the SID group than in the IC group (p < 0.05).
Table 3 Clinical symptoms and signs of 234 patients with pulmonary cryptococcosis of different immune statusNotably, 37.2% of patients were asymptomatic. This proportion was higher in the IC (42.6%) and MID (40.6%) groups compared to the OID (23.5%) and SID groups (18.2%) (p < 0.05).
Infection-related laboratory indicatorsAmong the 226 PC patients who underwent routine blood testing, inflammatory markers were variably elevated. Specifically, 32.4% of the 173 patients tested had elevated C-reactive protein (CRP), 44.7% of 114 patients had increased erythrocyte sedimentation rate (ESR), while procalcitonin (PCT) elevation was rare, observed in only 0.9% of 117 patients.
Additionally, (1,3)-β-D-glucan testing, performed in 95 patients using blood and/or BALF samples, revealed a positive rate of 37.9%. Galactomannan (GM) testing, conducted in 106 patients, yielded a lower positive rate of 6.6%.
Notably, the incidence of abnormal granulocyte counts was significantly higher in the SID group compared to the IC group (p < 0.05), although no significant difference was found between the SID and MID groups. No other significant differences were observed across immune status groups for the remaining laboratory indicators. Overall, inflammatory marker elevations were modest, with neutrophilia more commonly seen in patients with severe immunosuppression. (Supplementary Table 2).
Imaging changesHigh-resolution chest CT scans were performed in 234 patients prior to surgical or antifungal treatment. Among the 234 patients, 17.4% (39 cases) had single lesions, while 82.6% (185 cases) had multiple lesions. The lesions were predominantly subpleural in distribution, observed in 84.8% (190 cases) of patients. The most commonly affected lung regions were the lower lobes, with 55.7% (123 cases) involving the right lower lobe and 53.8% (119 cases) involving the left lower lobe. Notably, the incidence of left upper lobe involvement was significantly higher in the MID deficiency group compared to the IC group (p < 0.05).
Regarding lesion morphology, nodules were the most frequently observed lesion shape (78.6%, 176 cases), followed by patchy infiltrates (60.3%, 135 cases), and consolidation (12.2%, 28 cases). The most common concomitant signs were the halo sign (18.3%, 41 cases), mediastinal or hilar lymph node enlargement (12.9%, 29 cases), cavity formation (11.2%, 25 cases), and burr lobulation (6.3%, 14 cases). Representative chest CT findings for PC are provided in Supplementary Fig. 1. The relationship between immune status and chest CT features is shown in Table 4. The incidence of the burr lobulation sign was significantly lower in the MID group compared to the CO group (p = 0.008). The average short diameter of the largest lesion was 1.61 ± 1.0 cm (range: 0.05–5.5 cm), while the average long diameter was 2.73 ± 2.0 cm (range: 0.12–11.6 cm).
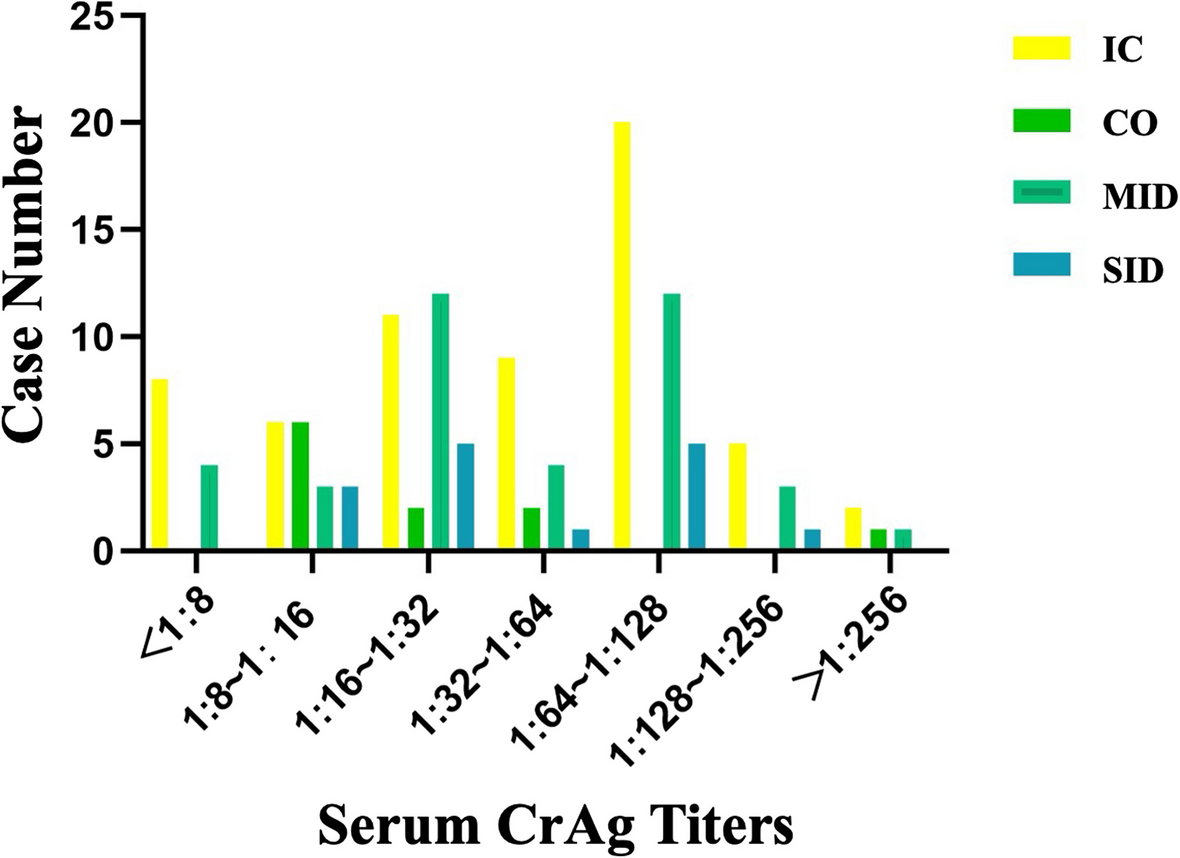
Table 4 Imaging features of pulmonary cryptococcosis patients with different immune statusCrAg resultsA total of 158 PC patients underwent qualitative CrAg test, which demonstrated a sensitivity of 94.9% (150/158). Of the eight patients who tested negative, seven were confirmed to have PC through histopathological biopsy, while one patient was diagnosed clinically based on additional quantitative CrAg testing, along with symptoms and imaging findings. The incidence of CrAg titers ranging from 1:8 to 1:16 was significantly higher in the CO group compared to the IC group (p < 0.05). However, no significant differences were observed between the CO group and other groups (Fig. 1).
Fig. 1
Cryptococcus capsular antigen titers in pulmonary cryptococcosis patients with different immune status
DiagnosisA total of 157 patients were pathologically diagnosed with pulmonary cryptococcosis. Among them, 106 cases were confirmed by CT- or ultrasound-guided percutaneous lung biopsy, 22 cases by transbronchial lung biopsy (TBLB) or bronchoscopic biopsy under direct vision, and 25 cases by surgical or open lung biopsy. Of these 25, two patients had positive metagenomic next-generation sequencing (mNGS) results for Cryptococcus neoformans from the same samples.
For one immunocompetent patient (IC group) originally diagnosed by CT-guided percutaneous lung biopsy, the diagnosis of cryptococcal infection was further supported by a positive culture for Cryptococcus spp. from purulent discharge of a skin infection. Four patients, all with severe immunodeficiency (SID group), had positive CSF CrAg results following lumbar puncture. These five patients were diagnosed with disseminated cryptococcosis. The rate of central nervous system involvement was significantly higher in the SIC group compared to the IC group (p = 0.011).
An additional 77 patients were clinically diagnosed with PC, all of whom tested positive for serum and/or BALF CrAg. Among them, two also had positive cultures from BALF, sputum, and/or tracheal aspirates; one had a positive mNGS result for Cryptococcus neoformans from a blood sample; and one had a negative culture result from pleural effusion samples.
The mean time from symptom onset to diagnosis among all 234 patients was 62.75 ± 100.66 days (range: 1–741 days), with no statistically significant difference across groups with varying immune status (F = 1.658, p = 0.177).
Treatment and prognosis analysisIn this study, the management of patients with pulmonary cryptococcosis (PC) generally adhered to the consensus recommendations of Chinese experts and the guidelines issued by the Infectious Diseases Society of America [15]. Treatment outcomes in relation to immune status are summarized in Table 5, with detailed treatment modalities and antifungal regimens provided in Supplementary Table 3. A total of 195 patients (83.3%) received only antifungal medication therapy, 20 patients (8.5%) underwent surgical as well as antifungal therapy, and 8 patients (3.4%) received surgery as the sole therapy. Eleven patients (4.7%) declined any form treatment. Among those receiving antifungal medication, 87.0% were treated with fluconazole, 8.8% with voriconazole, and two patients received amphotericin B combined with flucytosine followed by oral fluconazole. One patient was treated with fluconazole and flucytosine, followed by fluconazole, while another received fluconazole and caspofungin, followed by fluconazole. Three patients initially on fluconazole were transitioned to combination therapy with amphotericin B and 5-fluorocytosine due to central nervous system involvement. One patient was treated with amphotericin B and 5-fluorocytosine after no apparent response to fluconazole. Treatment durations ranged from 2 weeks to 3 years.
Table 5 Comparison of therapeutic effects in pulmonary cryptococcosis patients with different immune statusAt the time of the last follow-up, 135 of 158 patients were assessed for recovery or improvement. Of these, three were stable, three deteriorated, and four died.
Among all four deceased patients, one patient with existing hematologic malignancy died within 1 month of PC diagnosis. Another PC patient with solid malignancy died 3 months post-treatment. A third patient, diagnosed with disseminated cryptococcosis (central nervous system involvement), initially responded well to treatment but later died from pneumonia and multiple organ failure due to a bloodstream infection caused by listeria meningitis and diarrhea. These three cases were classified as non-cryptococcal infection-related deaths. One patient with disseminated cryptococcosis and hematologic malignancy died 5 days after treatment, and this death was considered related to cryptococcal infection.
Comments (0)