Characteristics of documents
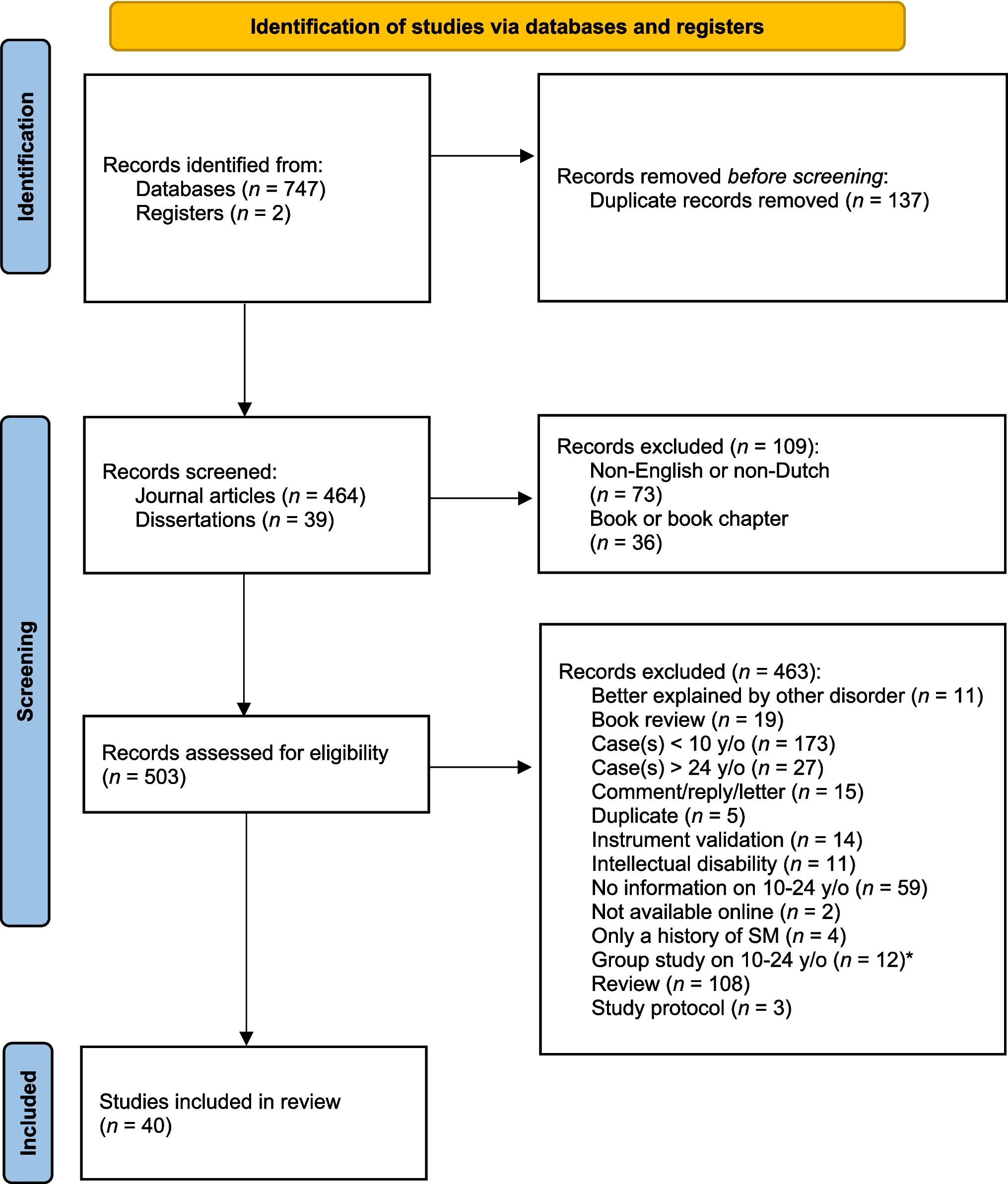
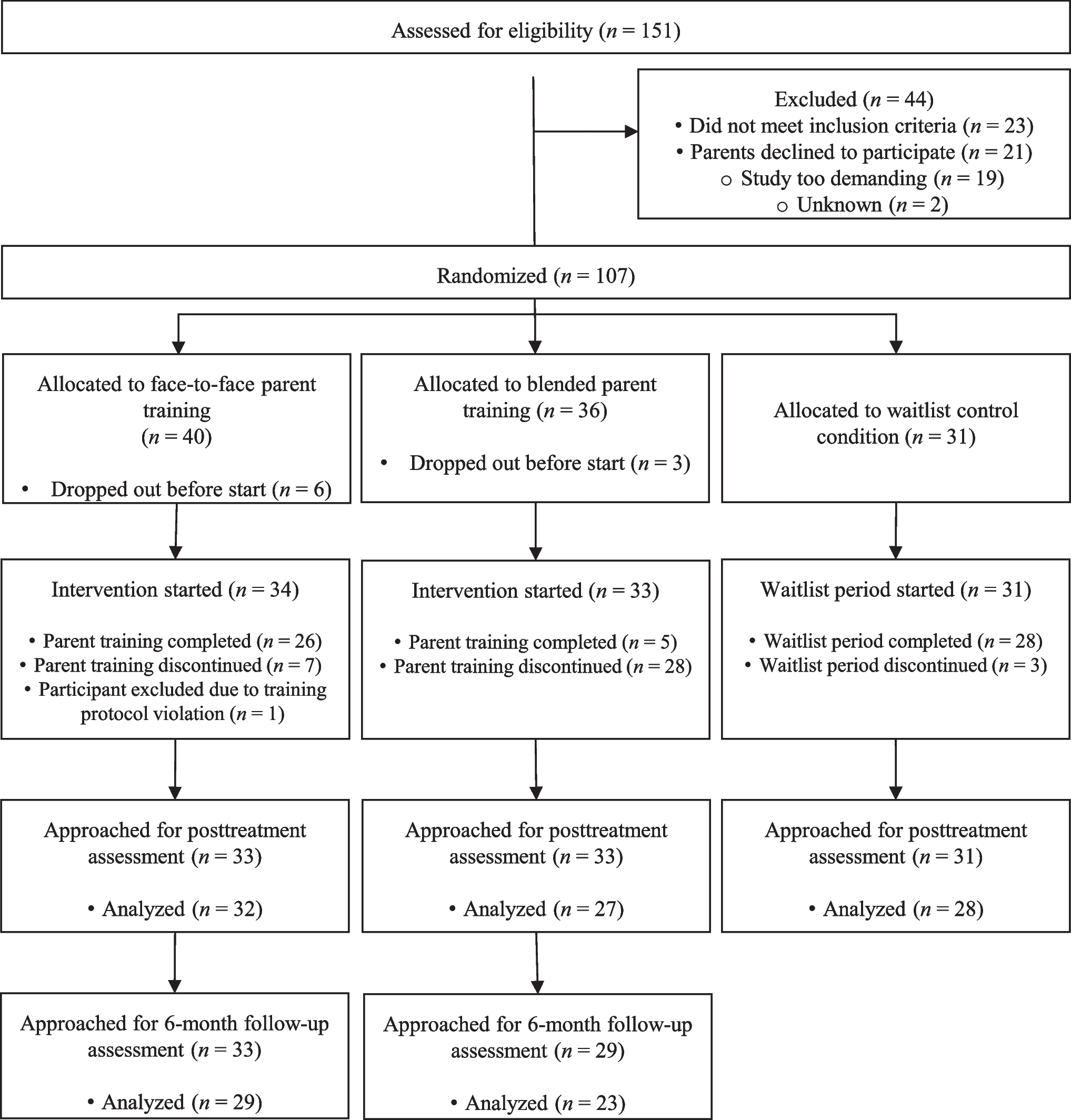
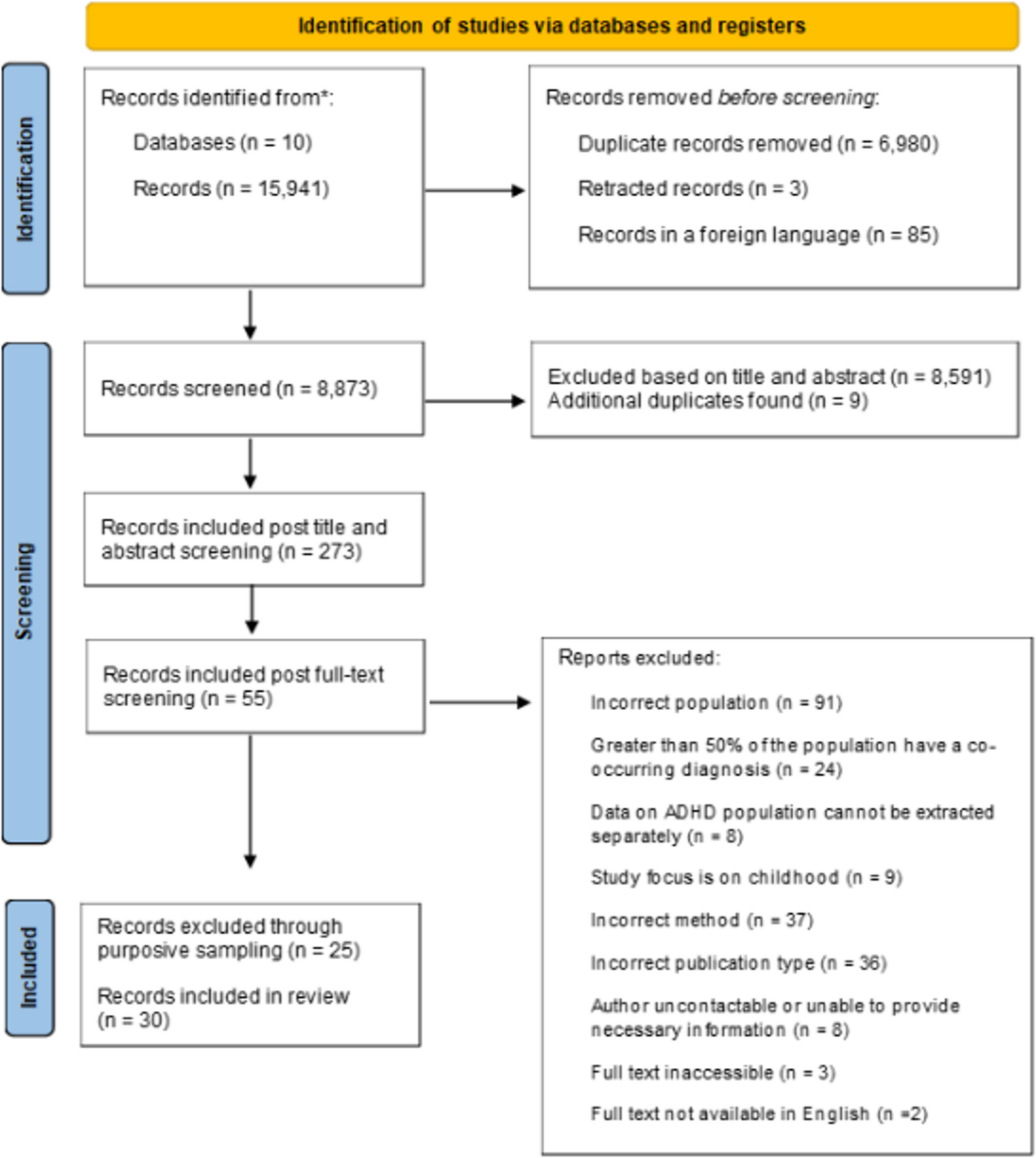
Search one and search two together initially yielded 11,433 articles for screening (see Fig. 1). Following title and abstract screening, 31 documents met al.l our inclusion criteria and were retrieved for full-text review. One document was identified through handsearching during the review process, following a suggestion from a peer reviewer [55]. Ten documents were ultimately included: six peer-reviewed articles and four grey literature documents, specifically dissertations. Two primary authors wrote four of the six peer-reviewed articles (two each). Two of these studies are related: Preyde et al. [7] was a quality improvement study aiming to improve school re-entry after psychiatric hospitalization, based on the outcomes of Preyde et al. [19]. The included documents were published between 1987 and 2024, with all but two published in 2017 or later. Four peer-reviewed articles were from the United States, and two were from Canada. Three of the dissertations were published in the United States, and one was from the UK. Six of the included documents used qualitative methodologies, and four used a mixed methods approach. Three studies explored this transition by capturing factors students perceived to be associated with positive school re-entry [7, 29, 56], and one captured factors associated with negative re-entry [19]. One study measured this phenomenon by investigating students’ perceptions of specific school-related factors that impacted suicidality during their transition back to school from psychiatric inpatient care [41]. Three of the peer-reviewed articles recruited participants with a range of diagnoses, including mood disorders, anxiety disorders, substance use disorders, etc [7, 19, 56]. Diagnoses were captured through self-report [7, 19], and/or obtained from participants’ clinical team [19, 56]. Three of the peer-reviewed articles focused on participants with a specific psychiatric presentation, the majority of whom had a history of suicidal thoughts and behaviours, identified through self-report [23, 57] or from medical records [41]. All but one of the documents focused on students between the ages of 9–20, and only one study recruited students younger than 12 years of age [58]. All the documents included information about sex and recruited both male and female participants. Three studies included information about participants’ gender identity [23, 41, 57], and three studies included information about their race and/or ethnicity [7, 23, 41]. Table 2 features the extracted characteristics of the included documents.
Table 2 Facilitators and barriers organized by the EST frameworkFacilitators and barriers
Facilitators were those factors students perceived to be helpful as they transitioned between inpatient psychiatric hospitalization and school, while barriers were those factors students perceived to have a negative effect on this process. A total of six facilitators and four barriers were extracted from the included documents and organized using the ecological systems theory framework. Interestingly, four of the facilitators were “positive opposites” [59] of each of the barriers, while the remaining two facilitators were distinct and did not have opposing barriers. These four pairs included one factor classified as related to students’ internal influences (i.e., psychiatric symptomology) [7, 19, 23, 30, 41, 55, 56], and three factors related to school support (i.e., connection to peers, connection to school adults, and academic planning and accommodations) [7, 19, 23, 29, 30, 41, 55,56,57]. Of the two distinct facilitators, one was related to family support (i.e., caregivers advocating for students at school) [19, 23, 29, 55], and one was related to school support (i.e., mental health supports at school) [7, 19]. There were zero facilitators or barriers related to hospitals or communities that were appropriate for inclusion based on our methods. Table 2 outlines each facilitator and barrier within the framework.
Internal influencesPsychiatric symptomology
Some students reported feeling calmer and more positive, and experienced fewer distressing symptoms after receiving inpatient care, which made it easier to be back in the classroom [19]. Other students felt they were better able to cope with their mental health issues and expressed both pride about their personal growth and hope for continued improvement [30]. Four of the included documents found that ongoing psychiatric symptoms were a barrier to students’ transition back to school [7, 19, 30, 55, 56]. Some students struggled with feeling connected to school and learning after psychiatric hospitalization due to overwhelming emotions [19, 23, 29, 55]. Students also found it difficult to juggle managing their symptoms while trying to keep up with their classes and coursework and reintegrate into their social circles [7, 19, 56]. Students reported that during the school reintegration period they struggled with feelings of anxiety [19, 30], emotional instability [19], and experienced decreased ability to focus [19, 30] when at school.
Family supportCaregivers as advocates
Some students perceived their parent(s’) or caregivers’ support as a facilitator to their transition back to school. Specifically, students found it helpful when their parents or caregivers advocated for their safe return to school by communicating with school staff about their hospitalization and negotiating the timeline for returning to classes [29, 41, 55]. These students reported that they also felt supported when parents or caregivers contacted their teachers to discuss academics, including making up missed work and planning for any necessary accommodations [29, 41].
School supportConnection to peers
Students who felt that they had the support of friends and peers often reported positive school reintegration [19, 29, 41, 55]. One student described her transition back to school as “pretty easy,” because her friends were there for her [30]. Some students found understanding and acceptance when they informed their close friends about their hospitalization and received both emotional and academic support (help with schoolwork) [19, 30]. One student reported that speaking openly with a peer who had also been hospitalized for mental health reasons was validating during his transition [30]. Conversely, some students reported experiencing discord within their friendships after hospitalization, and some found that certain friendships were lost during periods of hospitalization, leaving them feeling lonely and unsupported [19, 41]. Students also reported difficulties with peers asking them judgemental and intrusive questions about their absence from school [30, 41, 57] and spreading false rumours regarding the reasons behind their missed classes [7, 29, 30, 41]. Many students experienced bullying when they returned to school [7, 19, 23, 30, 41, 55], and some were specifically teased about their hospitalization [30].
Table 3 Characteristics of included documentsConnection to school adults
Students reported that having a teacher or other school staff intentionally reach out to them or “check up” on them upon their return to school positively affected their reintegration into the classroom [19, 30, 41, 55, 58]. One student shared that having school staff who were “really understanding” about their absence due to hospitalization made it easier for them to engage with school [30]. Some students also felt they gained support during their transition when they informed school staff, specifically teachers, about their mental health issues and hospital stay [19, 30]. Students reported that relational difficulties with school adults, especially teachers, made their transition back to school harder [23, 29, 30, 41, 55]. Some students felt that school staff did not have the capacity to support them with their mental health [29], while others felt judged and dismissed [30, 41, 55]. Marraccini et al. [23] found that students struggling with suicidal thoughts and behaviours who had higher negative perceptions of their relationships with teachers had more severe and intense suicidal ideation, and these effects were found to be greatest in the transitional period following hospitalization.
Academic planning and accommodations
Students appreciated when staff at their schools took the time to work with them to set expectations around school re-entry and develop a plan for reintegration; students wanted to feel that their needs were considered during this time [7, 29, 30]. They felt it was important that these meetings include a discussion around making up missed schoolwork, with clear communication from teachers about timelines for work completion [7, 30, 41]. Students found i

Comments (0)