Study information
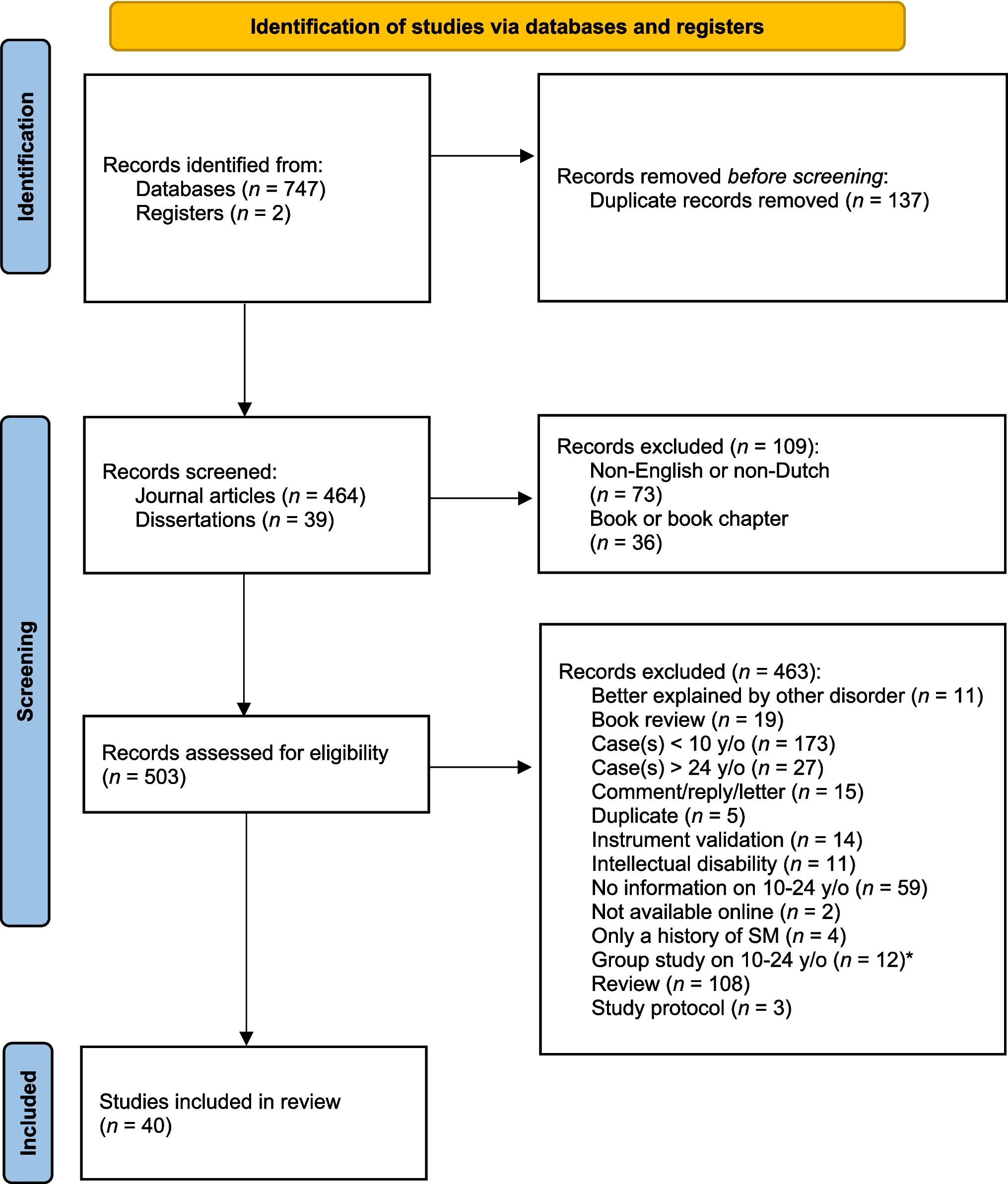
The included studies (38 published, 2 unpublished) are described in a schematized summary, shown in Table 1. The majority of the 40 included studies are case reports (n = 20, 50%) or case studies (n = 12, 30%) written from a therapist perspective (n = 30, 75%) and a cognitive behavioral theoretical approach (n = 13, 32.5%). According to the criteria used, three studies are of low quality (n = 3, 7.5%), while the majority is of medium (n = 26, 65%) or high quality (n = 11, 27.5%).
As shown in Table 1, the included studies contain 54 unique cases aged between 10 and 24 years (25 man (46.3%), 26 woman (48.1%), and 3 transgender (5.6%)), of which a majority of 36 adolescents was aged up to 15 years (66.7%). Twenty-five of the participants were seen in an out-patient setting (46.3%), thirteen in a research setting (24.1%), ten in an in-patient setting (18.5%), three in an education setting (5.6%), and three in another setting (5.6%). As shown in Table 2, SM was present when participants were on average six years old, but only got diagnosed at an average age of nine and a half years, indicating an average lag time of about three and a half years. The mean duration of SM was found to be seven years, and almost half of the participants suffered from a co-occurring condition besides SM (n = 24, 47.1%), with autism spectrum disorder (ASD, n = 11, 20.4%) and social anxiety disorder (SAD, n = 9, 16.7%) being most prevalent (see Table 1 for prevalence).
Table 2 Descriptive statistics of age related variables (in years)For the assessment of SM symptoms, semi-structured interviews were reported to be used in seven participants, including the Anxiety Disorders Interview Schedule for Children for DSM-IV (ADIS-IV-C/P; [1]) [12, 15, 21, 24, 32], the Schedule for Affective Disorders and Schizophrenia for school-age children-present and lifetime version (K-SADS-PL; [32]) [18], and one unspecified interview [4]. The Selective Mutism Questionnaire (SMQ; [8]) was reported to be used in three participants [12, 16, 25], while structured observation of speech behavior was reported to be used in six participants [4, 15, 17, 19, 24, 28].
Participant characteristics
Participant characteristics are summarized in Table 3. Difficulties or delays in early language production or processing were reported for twelve participants (22.2%). Second, problems in social interaction or with social relations were reported in almost half of the participants (n = 25, 46.3%), and often co-occurred with fear of or anxiety about social situations, reported in about one-fifth (n = 12, 22.2%) and one-third (n = 19, 35.1%) of the participants respectively. In line with this, a third of the participants were reported to avoid social interaction (33.3%). Also, two-fifth of the participants were reported to be shy (n = 22, 40.7%), either by showing an inhibited temperament from an early age (n = 13, 24.1%), and/or by withdrawing from unfamiliar situations or people (n = 14, 25.9%). In addition, for nine participants a negative affect was reported (16.7%). Despite the internalizing pattern described here, a quarter of the participants were reported to show disruptive behavior while growing up (n = 13, 24.1%).
Table 3 Reported participant characteristics with descriptions, frequencies (% of total participants (n = 54)*), examples, and relevant article numbersRegarding the etiology of SM, a positive family history of SM or extreme shyness was reported in ten participants (18.5%). In addition, parents or siblings of fourteen participants were reported to show (symptoms of) psychopathology other than SM (25.9%), like anxiety or depressive disorders. Traumatic life events like hospitalization or death of a close family member or pet, were reported in about a quarter of the participants (n = 15, 27.8%). However, only in eight participants these traumatic life events happened before the onset of SM [2, 16, 18, 20, 31, 34, 36]. Last, for two-third of the participants, SM was reported to be present in the school setting (n = 37, 68.5%), while for almost half of the participants SM was reported to be present with extended or non-family members in- or outside home (n = 26, 48.1%), and for ten participants SM was reported to be present with one or more core family members at home (18.5%).
TreatmentsPrevious treatment
Previous treatment efforts were reported in 29 participants and were (cognitive) behavioral or psychodynamic in nature and/or entailed adjustments in or outside the classroom with the help of special education services or a speech/language therapist. However, most of these previous treatment efforts were reported to be ineffective. Only the use of an selective serotonin reuptake inhibitor (SSRI) was reported to be a little effective in reducing SM symptoms before current treatment efforts [27].
Current treatment
Treatment duration was reported for 30 participants and ranged from one month to two years or 5 to 75 sessions, see Table 4.
Table 4 Treatment duration (for n of participants)Psychological interventions
The use of cognitive behavioral treatment (CBT) elements to treat SM was reported in 22 participants (40.7%). At the start of treatment, psycho-education was provided in ten cases to explain the rationale for treatment and to build rapport with the participants and their parents and/or teachers [5,6,7, 10, 12, 13, 16, 24, 25]. In addition, cognitive restructuring was used in four cases to identify and challenge distorted or irrational thoughts and beliefs, for example that the world, and speaking in it, is unsafe [12, 16, 25, 27]. Moreover, relaxation exercises like diaphragmatic breathing and progressive muscle relaxation to reduce arousal were used in three participants [2, 16, 25], while exposure exercises to feared situations to decrease anxiety and avoidance behaviors and increase speech behavior were conducted in fifteen participants [2, 4, 5, 7, 12, 15, 16, 18, 20, 21, 24, 25, 28, 30]. Also, social skills training to develop and enhance interpersonal skills and improve interaction with others was provided to nine participants [6, 13, 16, 19, 24, 25, 27, 28, 30]. Last, parent training to equip parents with the knowledge, skills, and strategies needed to effectively manage and support their child with SM was provided to the parents of five participants [4, 5, 14, 16, 24]. Contingency management to systematically reinforce desired speech behavior was incorporated into CBT for thirteen participants [4,5,6, 12, 15, 16, 19,20,21,22, 25, 27, 28] and offered as a standalone treatment (behavior therapy (BT)) in five participants [17, 33, 34, 36, 37].
Other psychological interventions reported were creative/art therapy to enhance self-expression in three participants (5.6%) [13, 14, 26], psychodynamic/play therapy to help participants express thoughts and feelings and understand their experiences in six participants (11.1%) [13, 14, 25, 27, 33, 36], and system/family therapy to address the relational dynamics and interactions within the participants’ family in nine participants (16.7%) [6, 7, 10, 23, 25, 27, 29, 34].
Pharmacological interventions
Pharmacotherapy was reported to be used to treat SM in 16 participants (29.6%). In all cases but two, an SSRI was prescribed to decrease anxiety symptoms and to increase speech behavior. In one case the SSRI was prescribed to improve depressive symptoms, and in this case the medication did have a positive effect on the individuals’ mood but not on the individuals’ SM [6]. In one case a tricyclic antidepressant was prescribed, with some improvements in mood and social interactions reported, although this participant was still unable to speak at school and with peers [32].
Primary treatment outcomes
In total, current treatment effects were described for two-thirds of the participants (n = 37; 68.5%). Of them, a total of 25 participants was reported to be SM diagnosis free post-treatment (67.6%), whereas nine participants were reported to still suffer from SM post-treatment (24.3%). For three participants the outcome of the described treatment efforts was not reported (8.1%).
In Fig. 2, treatment outcomes per specific treatment are shown. Some additional information is worth mentioning. First, out of the 17 participants who were reported to be SM diagnosis free after CBT treatment, the effect of only nine could directly be prescribed to the effects of CBT alone [2, 6, 15, 20, 21, 24, 28, 30]. In all other participants treated with CBT, it remained unclear whether treatment success was due to CBT or the combination with other interventions like pharmacotherapy [4, 5, 10, 12, 16, 27] or psychodynamic/play and/or systemic/family therapy [10, 25, 27]. Second, for two out of four participants who were reported to be SM diagnosis free after contingency management (behavior therapy), the treatment success could also be due to the use of play therapy [33, 36]. Third, in on

Comments (0)