
Remember me
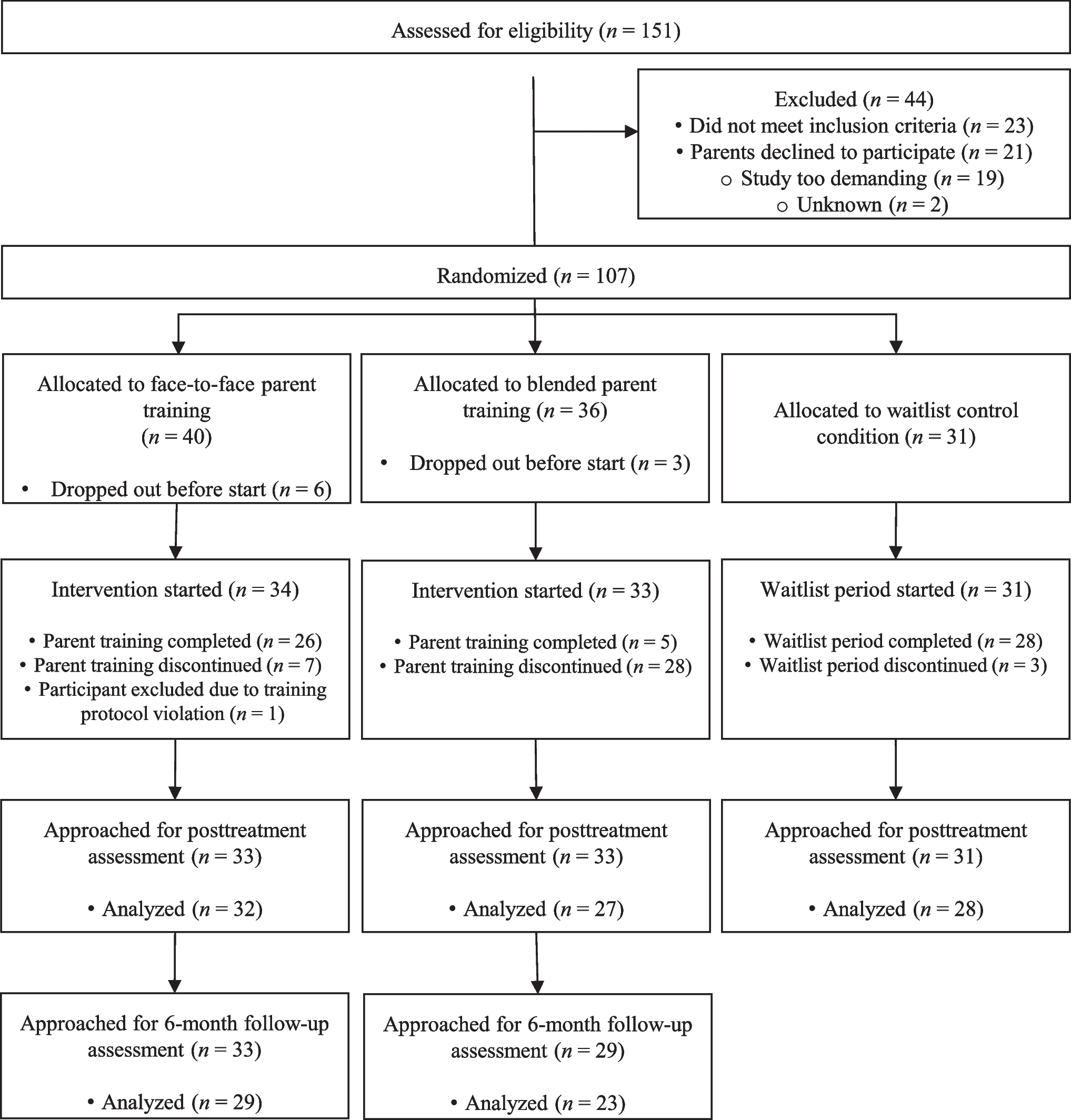
This two-center randomized controlled trial included parents of 97 children, randomized over three conditions: face-to-face parent training (n = 33), blended parent training (n = 33), or a waitlist control condition (n = 31). Details of the study design, procedure, and training content, have been published elsewhere [8] and are therefore only summarized in the current manuscript. For details on disruptive behavior outcomes, also see [8]. The trial has been registered in the Dutch Trial Register (see https://onderzoekmetmensen.nl/en/trial/22042.)
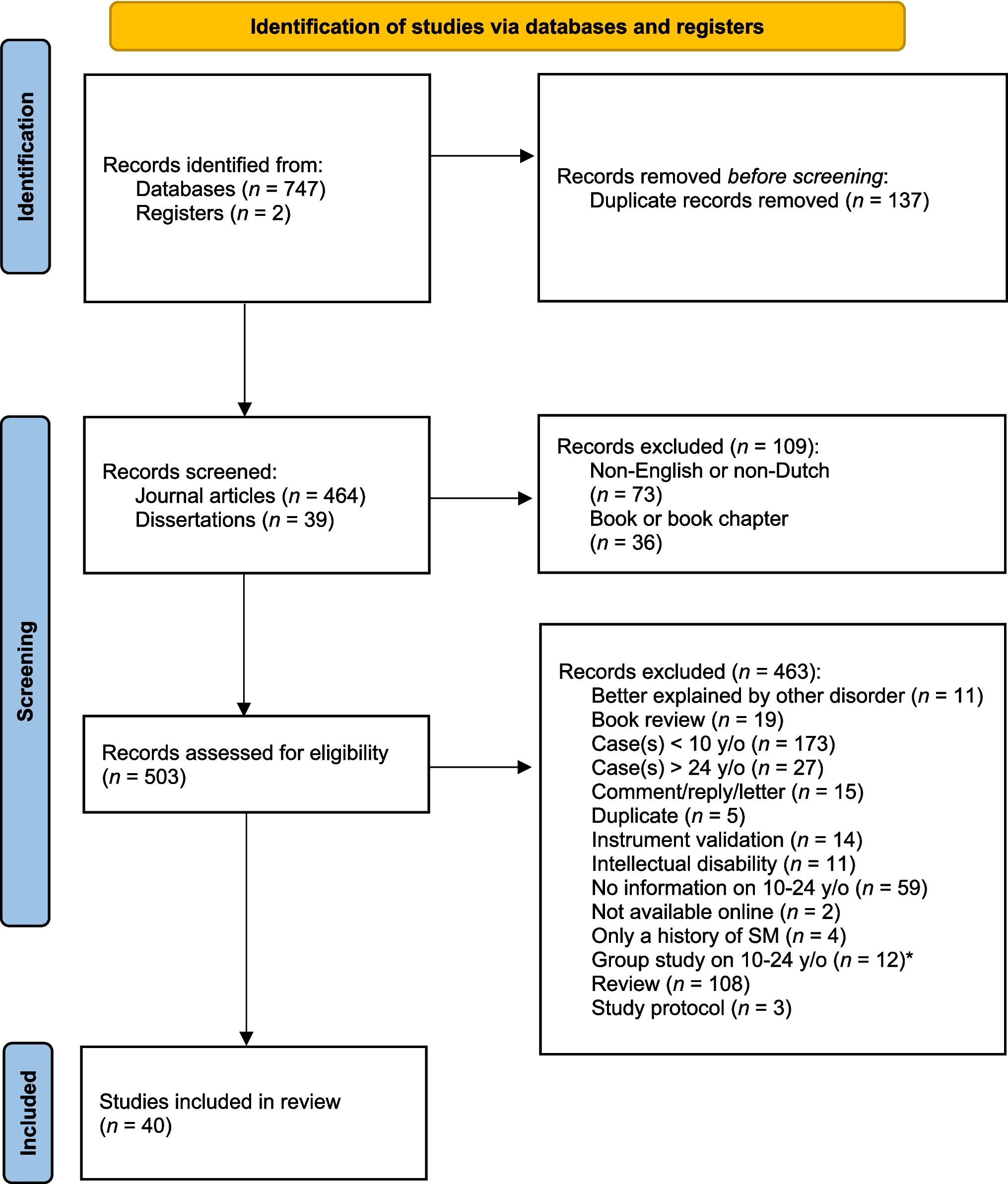
ParticipantsRecruitment took place between December 2014 and March 2018 from two outpatient centers for child and adolescent psychiatry in the Netherlands. Participants were included if the child: 1) had an Autism Spectrum Disorder diagnosis according to the DSM-IV-TR [4] or DSM-5[5]; 2) was aged between 4 and 13 years; 3) had a total IQ higher than 50; 4) did not use psychotropic medication or was on a stable dose for at least 6 weeks before study entry, with no expected changes during the study; and 5) had at least three parent-reported disruptive behaviors at home, as assessed by the list of target behaviors [44]. Furthermore, 6) at least one parent had to be willing to participate in the parent training; and 7) parents had to have a laptop or PC at their disposal. Exclusion criteria were the following: 1) the family required immediate intervention (e.g., families in which one of the parents was experiencing acute mental problems or in which the safety of the child could not be guaranteed); 2) parents had received parent training in the year prior to the study; and 3) the family intended to move to a region far from one of the study locations within six months. No restrictions were set to the child’s co-occurring mental health problems. For full details on participant flow, see Fig. 1. The study was approved by the Medical Ethics Review Committee of the University Medical Center Groningen.
Fig. 1 Procedure
ProcedureParents of potentially eligible children were invited by their clinician to participate in the study. If parents were interested to participate, we provided parents and children with more details about the study. If they agreed to participate, parents and children aged 12 or older signed informed consent.
Parents completed the baseline questionnaire online (also see Measures below). Participants were randomized after pre-assessment, and in the two training conditions families started with the parent training on average 47 days (SD = 20.38 days) after completion of the baseline questionnaire. At the start of the training, parents selected three to five problem behaviors and situations to be targeted in the parent training. Both the face-to-face and the blended training consisted of four phases: 1) introduction and psychoeducation; 2) techniques to change antecedents of problem behavior; 3) techniques to change consequences of problem behavior; and 4) evaluation and generalization.
Participants in the face-to-face training condition received the full training in a live setting with the same therapist, with sessions lasting between 45 and 60 min. Participants in the blended training condition completed the training through an online program with different modules in a set order. They received written feedback from a therapist on their exercises. In addition, they attended at least two face-to-face sessions (45–60 min) with a therapist, to evaluate their progress. Participants in the waitlist control condition went through a waitlist period of 20 weeks. In all conditions, children and parents were allowed to receive other (mental) health care, except for behavioral parenting interventions directed at the child’s behavior.
MeasuresAll measures were completed by the parents. For all but one participant, the parent who spent most time with the child attended the parent training (either alone or together with another parent) and the assessments of these parents were used for the analyses. For the outcome measures, we only used the subscales of each measure.
Demographics oChild. Parents reported their child’s age, sex, birth country, school type, IQ, autism severity, co-occurring mental health problems, and mental health care use (directed at the child).
oParent. Information was collected regarding the parent’s age, relation to the child, working situation, family composition, mental health care use (directed at the child), and several (self-reported) behaviors that will be published elsewhere.
Parent-related Measures Parenting sense of competenceThe Parenting Sense of Competence scale (PSOC [12]) contains two subscales: Parenting Satisfaction and Parenting Efficacy. The Parenting Satisfaction subscale consists of nine items and assesses the extent to which parents feel satisfied in their role as a parent (e.g., “Sometimes I feel like I’m not getting anything done as a parent”). Seven items constitute the Parenting Efficacy subscale, which assesses the degree of competence parents feel in their parenting role (e.g., “I honestly believe I have all the skills necessary to be a good parent to my child”). Items are rated on a 6-point scale ranging from strongly disagree (1) to strongly agree (6), with satisfaction items being reverse-scored. Subscale scores are calculated using the sum score of all items belonging to the respective (sub)scale. Higher scores indicate a higher sense of parenting satisfaction and efficacy. The internal consistency of the PSOC has been established (α = 0.75 and 0.76 for the Satisfaction and Efficacy subscales, respectively) [46].
Parenting stressThe Parenting Stress Index—Short Form (PSI-SF [1]) is a 36-item questionnaire comprising three subscales of 12 items each: Parental Distress, Parent–Child Dysfunctional Interaction, and Difficult Child. The Parental Distress subscale assesses the distress a parent experiences due to parenting-related personal factors (e.g., “I often feel tired, worn out, or exhausted from raising a family”). Parent–Child Dysfunctional Interaction measures the dissatisfaction parents feel regarding the interactions with their child (e.g., “I feel that my child isn't meeting my expectations”). The Difficult Child subscale assesses parents’ perception of their child’s manageability (e.g., “My child is more demanding than most children”). Parents rated each item on a 5-point scale ranging from strongly disagree (1) to strongly agree (5). A sum score is created for each subscale. Higher scores indicate more parenting stress. The internal consistency of the PSI-SF is good (α’s ranging from 0.80 to 0.91), test–retest reliability was high (r’s between 0.68 and 0.85), and the factor structure supported its validity [1].
Parenting styleThe Parenting Scale (PS [6]) assesses the degree to which parents use dysfunctional parenting styles towards their child. It comprises three subscales: Laxness (11 items), Overreactivity (10 items), and Verbosity (7 items). The Laxness subscale assesses the degree to which parents give in or allow their child to break rules (e.g., “When my child does something I don't like, I often let it go”). Overreactivity reflects the extent of displayed anger or irritability towards the child (e.g., “I almost always use bad language or curse”). The Verbosity subscale measures to what extent parents talk to their children to solve problems (e.g., “I give my child a long lecture”). Parents rated the occurrence of specific dysfunctional parenting behaviors on a 7-point scale ranging from never (1) to always (7). A sum score is created for each subscale, with higher scores indicating more use of the concerned dysfunctional parenting style. Internal consistency (α’s between 0.63 and 0.84) and test–retest reliability (r’s between 0.79 and 0.84) of the PS were adequate [6]. Although the PS was originally developed and validated in samples of parents of preschool-aged children, subsequent research has demonstrated that the measure is psychometrically sound and appropriate for use with parents of older children as well (e.g., [48]).
Child-related Measures Psychosocial functioningThe Strengths and Difficulties Questionnaire (SDQ [14]; Dutch translation [45]) was used to assess psychosocial functioning of the child. The SDQ contains 25 items rated on a three-point scale with the following anchors: 0 = not true, 1 = somewhat true, 2 = certainly true (reverse-scored for reverse-formulated items). The items are equally divided over five subscales: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behavior. The scores for each subscale are the sum of the individual items, resulting in a score from 0 to 10 on each subscale. Higher scores indicate more problems on the first four subscales and more prosocial behavior on the latter subscale. Internal consistency of the Dutch SDQ is acceptable (α’s between 0.57 and 0.81 for the parent report version) [45].
Adaptive behaviorWe assessed the child’s degree of adaptive behavior with the Vineland Adaptive Behavior Scales II (VABS-II [39]). The VABS-II contains 383 items describing behaviors across four subscales: communication (99 items), daily living skills (109 items), socialization (99 items), and motor skills (76 items; only until the age of 6). Given that the study also included children older than 6, the motor skills subscale was not assessed in the current study. Through an interview with parents, the administrator rated the occurrence of the behaviors on a three-point scale (0 = child never or very seldom performs said behavior, 1 = child sometimes performs said behavior, 2 = child usually performs said behavior). All subscales have age-standardized normative scores with a mean of 100 (SD = 15). Higher scores indicate more adaptive behavior. Given that no Dutch normative scores are available, we used normative scores of the United States [39]. Internal consistency of the VABS-II was good, based on split-half reliability and the Spearman-Brown prediction formula (across varying ages), r’s ranged from 0.84–0.93.84.93 for communication, from 0.86–0.91.86.91 for daily living skills, from 0.84–0.93.84.93 for socialization, and from 0.77–0.90.77.90 for motor skills [39].
Data AnalysisBaseline characteristicsTo test for differences between conditions on baseline characteristics, we conducted one-way analyses of variance for the continuous variables, and Chi square tests for the categorical variables, with condition (face-to-face, blended, waitlist) as the independent variable.
Baseline to posttreatmentWe tested the effects of both parent training formats (versus waitlist) in two separate linear regression analyses for each outcome, leading to a total of 16 regression models. That is, we calculated difference scores (posttreatment – baseline) of each outcome measure to include as the dependent variable. Each parent training format was compared to the waitlist condition separately. Two dummy variables for condition were included in each model: face-to-face (1) versus waitlist (0) and blended (1) versus waitlist (0). In line with Breider et al. (2024), we analyzed data on an intention-to-treat basis: all participants with posttreatment data were included in the analyses, regardless of completion status.
As children’s age may influence both parenting behavior and child (mal)adaptive behavior in children with autism (e.g., [15, 25], also see [8]), we added age as a covariate in all regression models. Moreover, to control for baseline differences and in line with our previous study [8], scores at baseline on the respective outcomes were also included as covariates in each model [43]. We assessed homogeneity of regression slopes by including interaction terms of the independent variables (age × condition dummies and baseline scores × condition dummies) in the model. Significant interactions were kept in the final model after centralizing the respective variable.
Baseline to 6-month Follow UpGiven that the waitlist condition started with parent training after the 20-week waitlist period, 6-month follow-up data were only available for the two parent training conditions. Hence, we tested follow up changes within each parent training condition with linear regression analysis, using the difference score (follow up – baseline) of each outcome measure as the dependent variable. We included age and baseline scores as covariates.
All analyses were performed with IBM SPSS Statistics version 27, with α = 0.05. We used Benjamini–Hochberg multiple testing correction to control the false discovery rate across the 16 regression models [7]. Adjusted p-values are reported.
An a priori power analysis, as described in our primary outcome study [8], showed that 118 participants (40 in the active conditions and 38 in the waitlist) were required to reach 80% power to obtain an effect of 0.65 on the primary outcome measure (based on Aman et al. [3] and Solomon et al. [38]).
Comments (0)