
Remember me
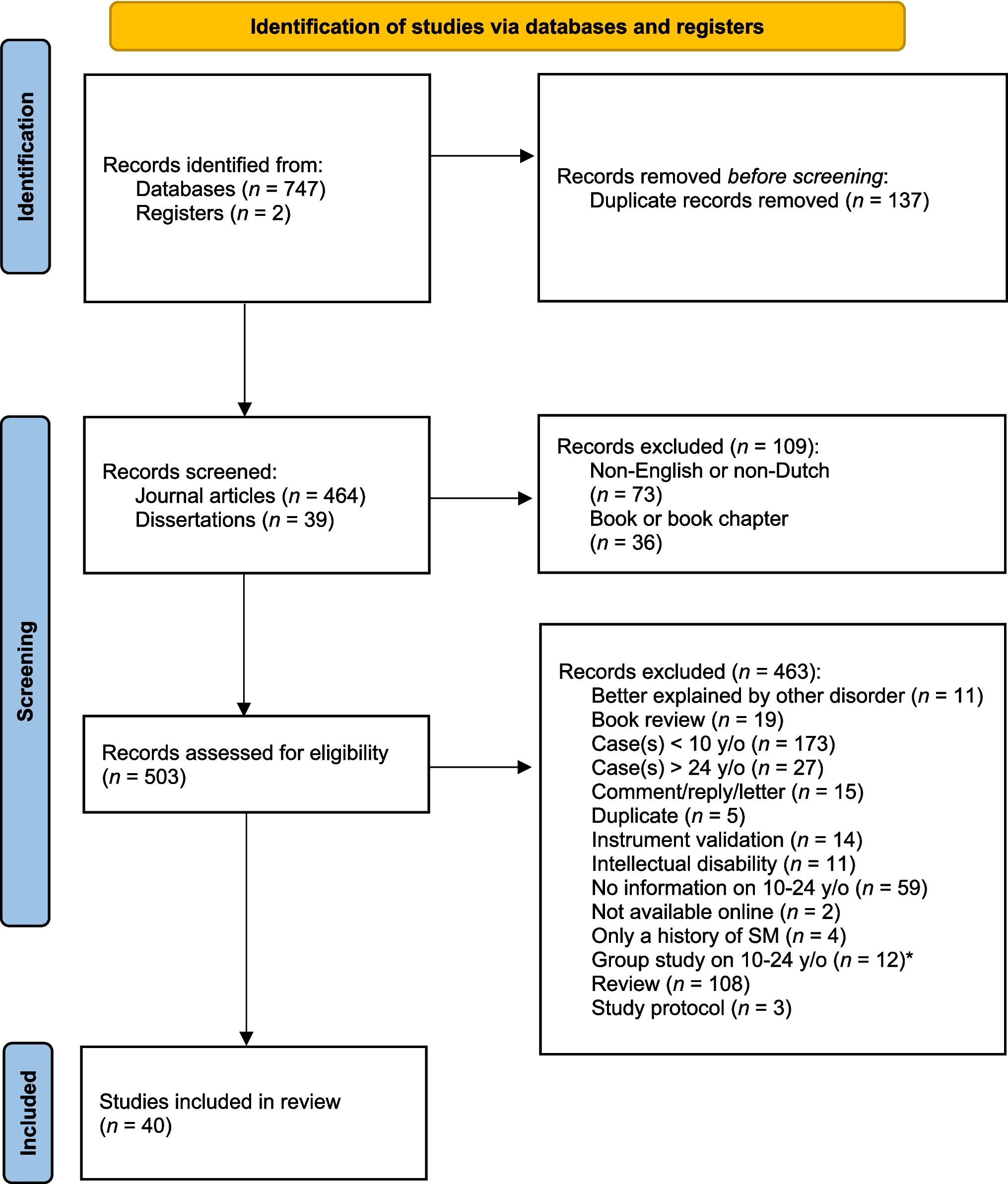
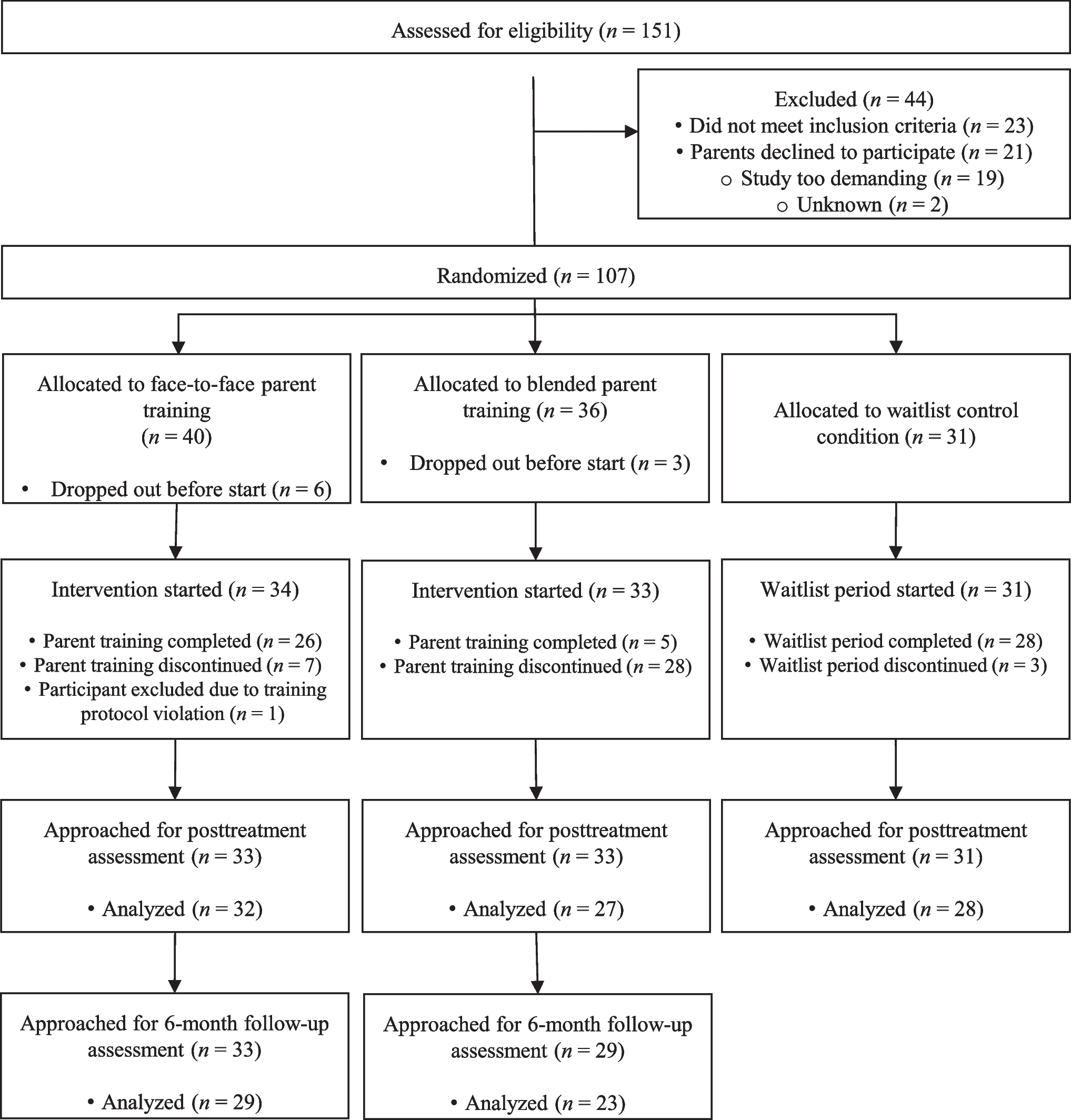
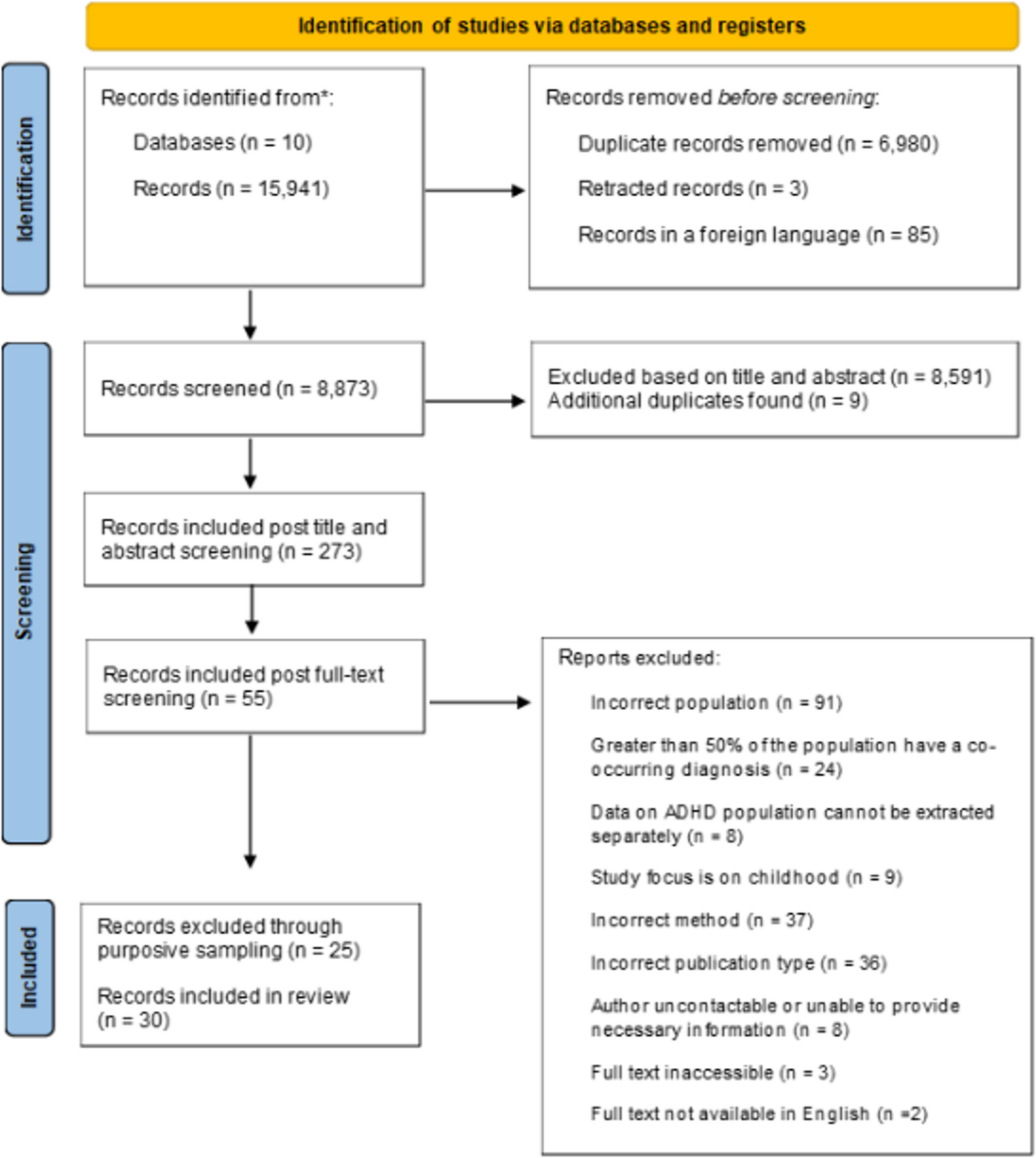
The study selection process is illustrated in Fig. 1. Following full text review fifty-five papers met the study inclusion criteria and these were reviewed to sample for maximum variation by dimension of lived experience. This led to the inclusion of studies which, for example, were the sole study focused on sport [53], weight-management [54] and primary care provision [55]. The studies with the highest (28.6 years) [54] and lowest mean age (15.1 years) [56] were also included as part of this process. The remaining studies were selected due to their data richness and alignment with the study scope. In total thirty papers were selected for inclusion.
Fig. 1
A PRISMA flow diagram illustrates the study selection process [57]
Summary of characteristicsThe thirty included studies report the experiences and perspectives of 805 ADHD youths (295 women, 478 men, one non-binary participant, one who preferred not to disclose gender, and 30 participants for whom gender data was not collected/reported). The mean age across studies that reported this information was 21 years. Of the 805 participants across the thirty studies, all but twenty-nine had a formal diagnosis of ADHD. Across studies, medication usage was reported in seventeen studies and revealed three varied patterns of medication use, daily use, occasional use and discontinued use. Non-pharmacological treatments, such as counselling, behavioural therapies, skills training, psychoeducation, and occupational support, were accessed by some or all participants in twenty-one studies (see supplementary file 6).
All included studies were published between 2006 and 2024 and were conducted across eleven countries, including the United States of America (11), Israel (4), the United Kingdom (3), Canada (2), Denmark (2), Norway (2), Korea (1), China (1), Ireland (1), Australia (1), North America (1), and Sweden (1).
Participants were mainly recruited through post-secondary educational settings and healthcare services, alongside liaising with ADHD organisations and utilising online fora. Semi-structured interviews were the most common data collection method, employed by twenty-six studies, one combined semi-structured interviews with focus groups, two used surveys employing phenomenological questions, and one utilised solely focus groups.
The focus areas of included studies can be categorised into experiences and perceptions of education (10), ADHD medication (5), living with ADHD (5), service provision (3), employment (2), emotional dysregulation (1), sport (1), stress (1), weight management (1) and substance use (1).
Quality appraisalThe results of quality appraisal of included papers are presented in supplementary file 5. No studies were excluded based on their quality, as all contributed valuable and important information regarding the research question, however just 4 of 30 studies received a positive score for every criterion.
ThemesThe analysis generated seven themes, or third-order constructs: (1) Navigating identity and authenticity (2) Diagnosis disclosure dilemma, (3) New ADHD manager reporting for duty, (4) The power of others, (5) Diverse healthcare journeys, (6) Impact on engagement in everyday activities, (7) Turning insight to action: application of self-help strategies. These themes, the number of studies relevant to each theme, and their key concepts can be found in Table 1.
Navigating identity and authenticityThirteen papers delve into the impact of ADHD on youths’ identity formation and authenticity. Many youths identify ADHD as integral to their identity and sense of self [58,59,60,61,62], aptly described metaphorically in one study:
“ADD does not describe me, it is me ….it’s not just two or three things about me. It’s like an octopus cause it has tentacles into every single aspect of me …I’m ADD. It affect[s] everything.” [61].
Some participants reported being unable to even imagine who they would be without ADHD [58,59,60]. Four studies described youth’s feelings of authenticity when they can experience and express their true identity, unmedicated [56, 58, 60, 63]. In a small number of studies ADHD medication was described as diminishing the exuberance that is part of their identity [56], creating a dilemma: to sacrifice their authenticity by using medication to enhance functioning, or to remain true to their identity going unmedicated [63].
Many studies described the impact of ADHD as a gift while others described it as a flaw negatively affecting their identity [56, 58, 60,61,62, 64,65,66,67,68,69]. Some youths appreciated the unique strengths it brings [56], such as creativity [56, 58], energy [58], individuality [66], sensitivity, empathy, insight [61] and outgoing characteristics [61, 62, 66].
Attaining an ADHD diagnosis was described in one study as empowering, providing validation and explanation for day-to-day challenges [64]. However, five other studies reported that youth find little meaning in attaining a diagnosis due to doubt surrounding its validity [56, 59, 62, 68, 69]. Furthermore, some youths struggle to connect their everyday experiences with ADHD characteristics [56, 59, 68], as described by one youth who does not experience inattention when the topic interests them:
“an ability not to have an attention span for very long. But I can have an attention span for extremely long for the things that I care about.” [68].
The diagnosis disclosure dilemmaEleven papers detail the complexities of disclosing ADHD [53, 56, 59, 61, 62, 64, 66, 70,71,72,73,74]. Youth report refraining from disclosing due to negative associations and stigma [62, 64, 66, 71, 72] gaining a sense of control by selectively sharing their diagnosis [70] or seeking to protect themselves from misunderstanding, judgement and rejection [64]. This creates a dilemma:
“There is a dilemma between keeping ADHD a secret to prevent stigmatisation, and at the same time longing for understanding from peers, colleagues and superiors.” [72].
Some youths chose not to disclose in education settings as they did not feel they required assistance [71] or because they wanted to be treated the same as classmates [74]. While youth may disclose their diagnosis with the expectation of receiving supports or accommodations [71, 74] this is not always realised. Two studies describe challenges obtaining formal supports in university settings [61, 71]. In two studies, youth grappled with disclosure due to the risk of their confidentiality being compromised to classmates [61, 65].
“One time I even got [my accommodation letter] out before class and three different people passed it around, and I was like, “Excuse me. Hello. That’s mine”. Yeah, they’re [sic] like, “Ooh, what’s this? Ooh, I need to get me one of these forms. Then I’ll be a good student.”” [61].
Two studies described disclosure in employment settings leading to youths’ ADHD characteristics being viewed positively [59] and receiving understanding and support from colleagues and superiors [72].
In team sports, youth felt compelled to disclose their diagnosis to coaches and teammates, to prevent misunderstandings and foster compassion [53]. Describing disclosure to coaches and teammates one participant reported:
“I am very verbal about it, having the problem. I let people know. Definitely. Because if you don’t let them know they are just going to be on you.” [53].
Diagnosis disclosure in friendships varied from those who openly share their ADHD diagnosis with friends [56, 61, 73], to those who feel comfortable only confiding in close friends [62] and in one study some participants reported they prefer to keep their diagnosis private [61].
New ADHD manager reporting for dutyEleven articles document youth’s experiences and perceptions of transitions from adolescent to adult [56, 60,61,62, 65, 69, 74,75,76,77,78] inclusive of experiences of transition from school to college [60,61,62, 69, 74, 76,77,78] and from child to adult health services [56, 60, 75, 77].
Entering college can be unsettling for youths [69], as they face a gradual increase in academic demands and responsibility for managing ADHD independently without parental support, which some perceived as a reasonable reflection of their maturation and growing independence [62, 74], while others enter college feeling unprepared to manage ADHD independently [62]. Parents who advocated for the youth by disclosing disabilities to teachers and assisting with schoolwork, offered immediate support but hindered their development of self-advocacy skills [62] with some youth in college just beginning to understand the importance of self-advocacy skills and their role in managing ADHD [74] and some feeling shocked when responsibilities shift [77].
“And now I’m like trying to take care of this all on my own just for me like just to take care of my own self I’m like wow, like it’s I didn’t realize like how much it is to deal with life with ADHD.” [77].
Similarly, the transition from child to adult healthcare services presents increasing responsibilities and challenges, with youth having varied perceptions of their readiness [60]. Their sense of preparedness is shaped by their knowledge of the process, feelings about adult services, and familiarity with them [
Comments (0)