The present study was approved by the Ethics Committee of the University of Freiburg (EK 124/17; PI CK) and all participants or their caregiver gave their informed written consent.
Participants
After the exclusion of participants for technical reasons (see data analysis below), the study sample included n = 139 participants, of which n = 65 had an ADHD diagnosis and n = 74 were neuro-typically developing, recruited through the departmental data base, for patients: if they fulfilled ICD-10 diagnostic criteria for ADHD (F90.0/1; ascertained from expert clinicians via anamnestic interviews, behavioural observations, and Conners’ parent and teacher rating scales), but did not present with the following co-morbidities, Autism Spectrum Disorder (F84), Schizophrenia or paranoid disorder (F20-F29) and for controls: if they had no psychiatric or neurological diagnoses. For all participants, exclusion criteria were IQ < 70, neurological disorders in the past and at present as well as eye-sight impairments (unless corrected). ADHD patients on stimulant medication (n = 20) refrained from taking these drugs for > 24 h before testing. For this sample, the power for the detection of a medium effect of d = 0.5 at alpha=0.05, one-tailed, was 0.90 (G*Power 3.1.9.6; Faul, 2020).
The ADHD sample was aged 13.1±2.4 years (range: 9;2–17;1ys), had an average IQ of 101±12 (range: 75–136), and included 25 females (38.5%). Neurotypical controls were aged 14.1±1.8 years (range: 9;1–17;3ys), had an average IQ of 120.1±17.4 (range: 73–160), and included 41 females (55.4%). Controls were somewhat older than patients (t = 2.48, p = .015), included more females (t = 2.01, p = .046) and scored higher in IQ (t = 7.66, p<.001).
Procedure
Individual testing sessions took place in the departmental eye tracking lab (sound-attenuated Faraday cage), lasted for about 150–180 min, comprised of overall 11 different eye movement tasks (order counterbalanced) and included breaks after every task. Stimuli were generated with the software package Experimental Builder (SR-Research, ON, Canada). Brightness within the Faraday cage was measured (Peaktech 5035) and kept constant at 70-80Lx.
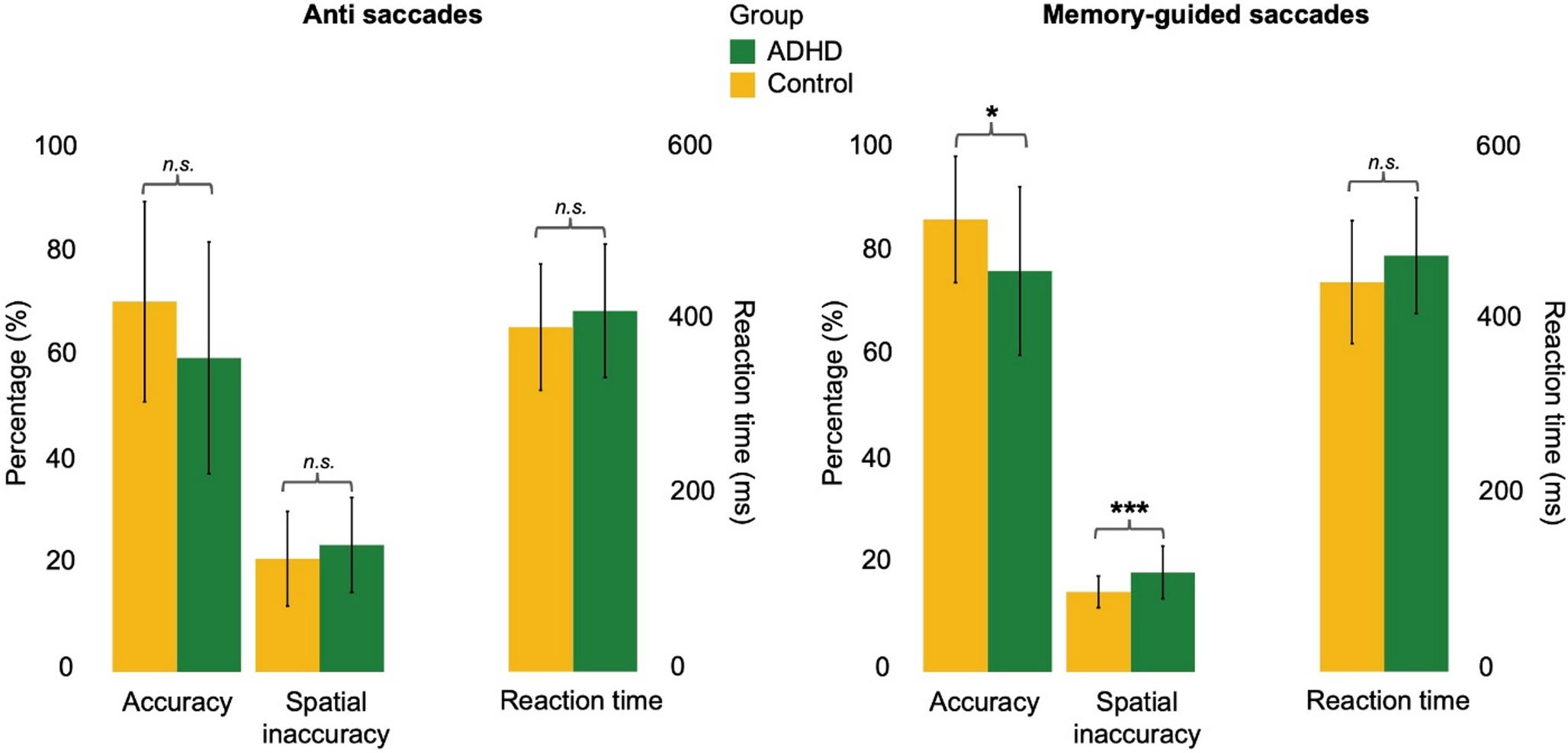
For the Memory-Guided Saccade task (“MGS”) an initial central fixation point was presented for 1,000ms, followed by an additional red circle presented horizontally for 100ms at one of the following pseudo-randomly sequenced positions to the left or right (±2.5°, ±5.0°, ±7.5°, ±10.0°, ±12.5°, ±15.0°) of fixation. After a memorization gap of 2,500-4,500ms, the central fixation cross disappeared, and after another 1,500ms the red circle re-appeared and stayed on screen for 1,000ms. After an inter-trial interval (ITI) of 1,000ms, the next trial began. Participants were instructed to remain with their gaze on the central fixation, remember the peripheral position of the red circle and look at this position upon the disappearance of the central fixation. Six practice trials preceded 48 test trials.
For the Anti-Saccade task (“AS”), each trial began with the presentation of a central fixation cross, followed 1,000ms later by a green circle presented in pseudo-random order at 7° to the left or right of fixation and remaining there for 1,000ms. After an ITI of 1,000ms, the next trial began. During the overlap condition, central fixation stayed on while the peripheral cue was visible; during the gap condition, central fixation was set off 200ms before the onset of the cue. Participants were instructed to look at the central fixation cross and look straight to the opposite-site mirror-image position of the cue upon its appearance (see [14]). Eight practice trials preceded 100 test trials.
The IQ-testing constituted a second session with groups of up to 8 participants and employed the CFT-20R [40].
Apparatus
Eye movements were recorded with the EyeLink1000 + eye tracker (SR-Research, ON, Canada), employing a 1000Hz sampling rate with 0.01 degrees resolution. Stimuli were presented on a 24’’ LCD-screen (1920*1080 pixels, 60 Hz refresh rate, viewing distance 90 cm). A 9-point-calibration preceded each task and subsequent drift corrections were accomplished as required. Recordings were recalibrated whenever necessary.
Data analysis
Primary data analysis (parametrisation) was accomplished for only one eye per participant, namely the one with better technical data quality according to the test protocols. Only saccades faster than 25°/s and larger than 1° were analysed, excluding micro-saccades [22]. Trials with eye lid closures or head movements were excluded. Only horizontal saccades were included.
Spatial inaccuracy of correct AS and correct MGS was defined as percentage error in amplitude (“PEA”) according to Mostofsky et al., [30]: PEA = 100*│1 – (eccentricity of final saccadic landing point [°] / eccentricity of target stimulus [°])│.
The first up to three saccades directed at the target (primary saccade plus two corrective saccades) were considered to derive the PEA measures. In about 57–63%, the first saccade reached a position closest to the target; in about 31–35% of the trials, this position was reached with the second and in 5–8% with the third saccade. This grossly summarized result held for both groups (AS: all ps>0.08; MGS: all ps>0.22) and both tasks (see minima/maxima above).
Reaction time was defined as the time between stimulus presentation and saccade onset for AS and as the time between the disappearance of the central fixation cross and saccade onset for MGS. For the derivation of correct AS, only saccades with reaction times 131–1000 ms post cue-onset were used.
Direction errors in the AS task were primary saccades with regular reaction times directed towards the cue. Accuracy was defined as the proportion of correct AS and MGS. At least 20 or 18 correct AS or MGS, respectively, were required for a participant to be included in the data analysis [5, 10].
A total of 12 subjects (N = 8 ADHD group; N = 4 control group) had to be excluded from the initial sample of 147 subjects (N = 73 ADHD group; N = 74 control group). Three subjects from the ADHD group were excluded due to missing data for one or both tasks due to discontinuation or non-performance. Another three subjects from the ADHD group were excluded for not reaching the specified minimum number of 20 anti-saccade trials (20%). As part of the statistical outlier adjustment (one and a half times the interquartile range), 4 subjects (N = 1 ADHD group; N = 3 control group) were excluded for MGS and 2 subjects (N = 1 ADHD group; N = 1 control group) were excluded for AS.
ANCOVAs used GROUP (ADHD vs. control) as a between-subject factor and included age, sex and IQ as co-variates. Leaving out sex and IQ as co-variates did not principally alter the results; leaving out age reduced between-group differences slightly. Furthermore, we correlated AS and MGS parameters co-varying for age, and determined their relationship with age (employing univariate linear regression). Finally, in order to assess whether the correlation between the spatial accuracies of AS and MGS changes with increasing age, we correlated the individual products of z-scores for AS and MGS (zAS * zMGS) with participants’ ages (see [20]). A zero correlation of this z-score product and age would suggest age-invariance of the relationship between AS and MGS spatial accuracy. Two-tailed p-values are reported throughout.

Comments (0)