Study characteristics
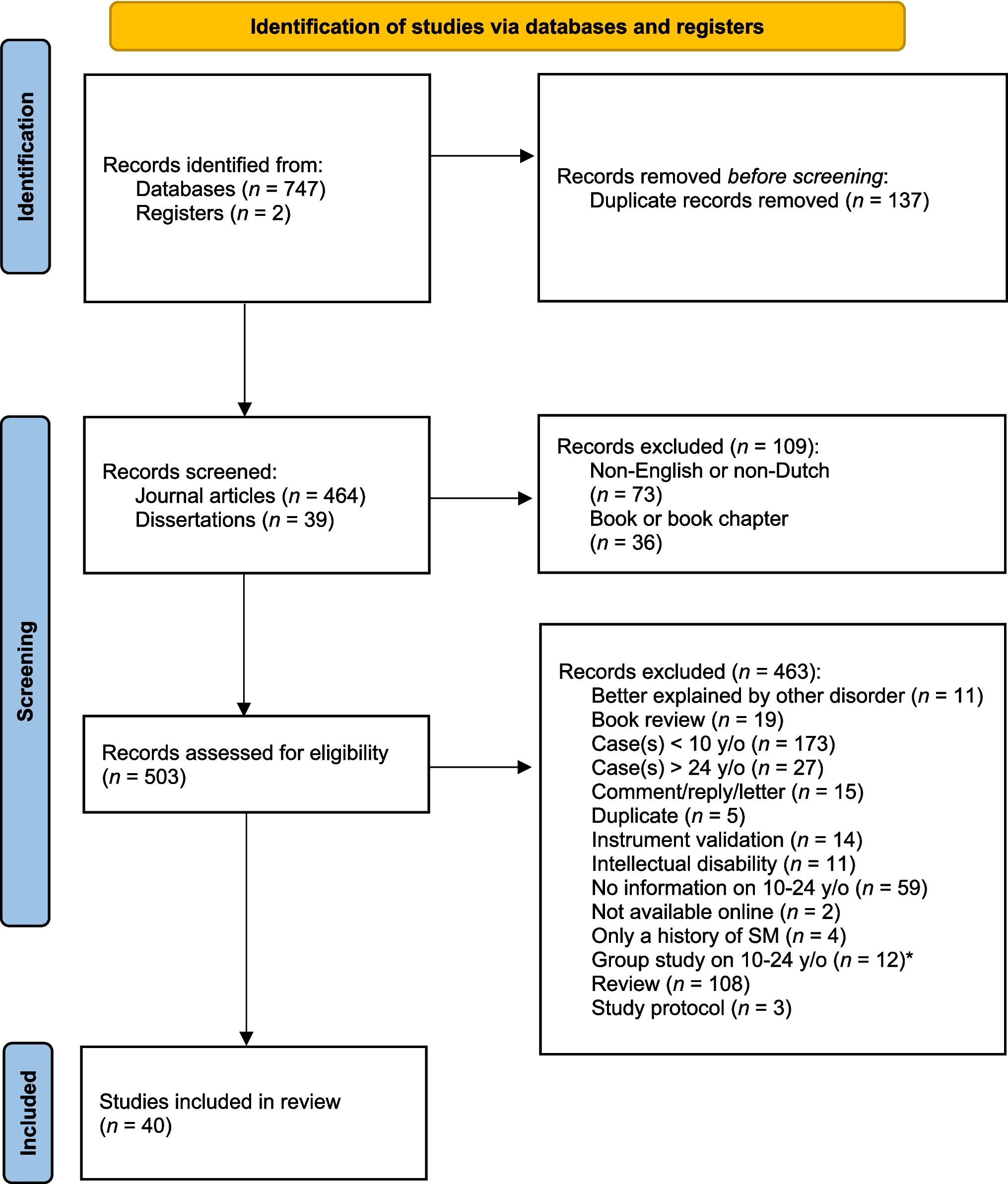
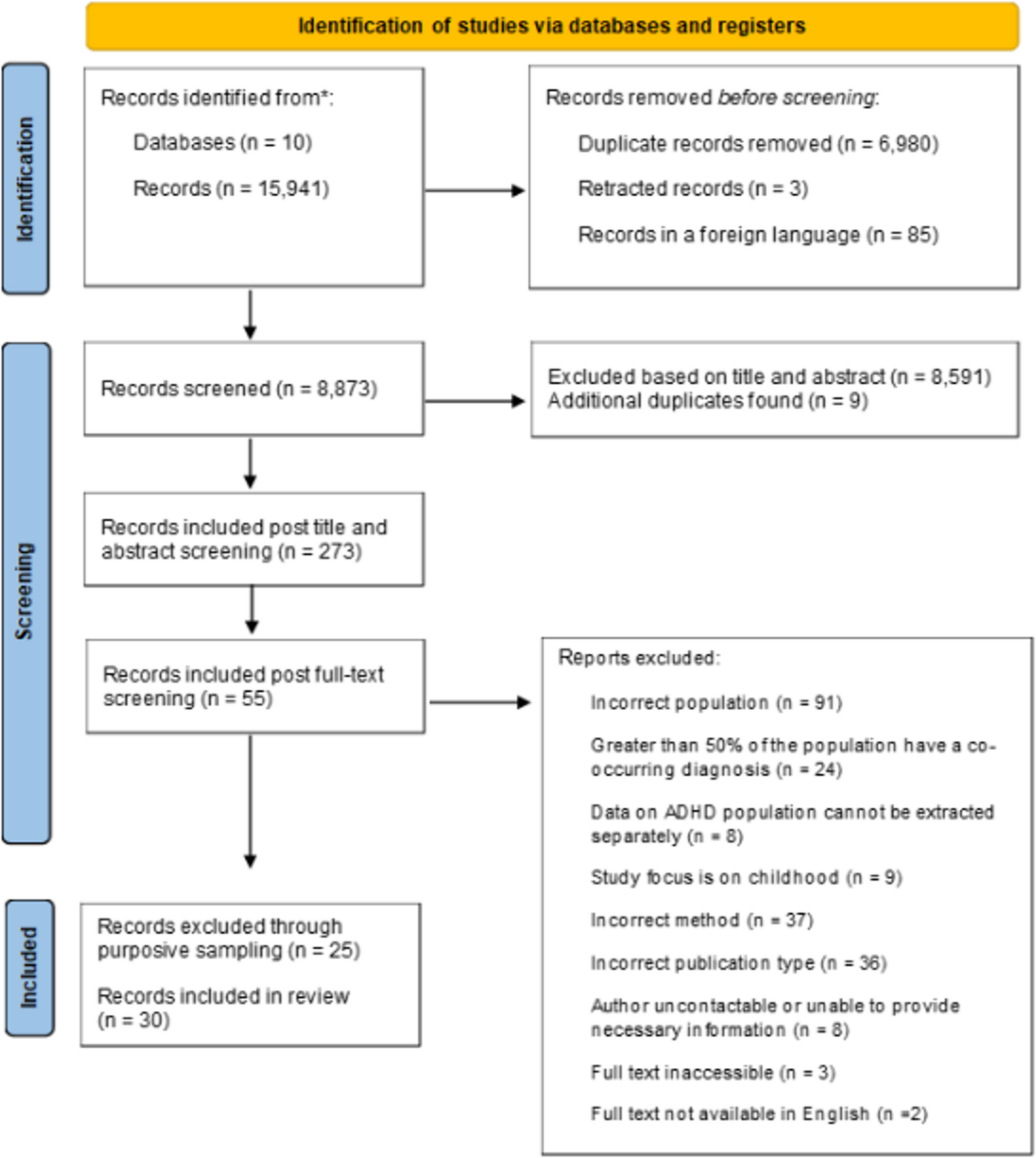
This review included 51 studies − 36 cross-sectional and 15 longitudinal − mostly conducted in the USA and UK. The studies covered samples across a wide age range, mainly focusing on early to middle childhood, with some also including adolescence and multiple age stages. Sample sizes varied significantly, from 17 to 10,438 participants (M = 892, SD = 2,055). Most studies showed a male gender imbalance, with male participation ranging from 44% to 88.2%. The majority of studies addressed a wide range of ID severities, covering at least three levels (e.g., mild, moderate, and severe). However, 14 studies did not specify the severity level of ID. Four studies (8.2%) focused on specific syndromes, such as Down and Fragile X syndrome (FXS). Regarding mental health problems, the most common were behavior problems (n = 16), followed by ASD symptoms (n = 14), unspecified psychopathology (n = 9), internalizing and/or externalizing problems (n = 7). Less common were anxiety (n = 3), depression (n = 3), conduct disorder (n = 3), hyperactivity (n = 2), ADHD symptoms (n = 2), emotional problems (n = 3), and maladaptive behavior (n = 2). Notably, 37 out of 51 studies (72.5%) used only univariate analyses, and no qualitative studies were identified in the search. Critical appraisal classified 19 studies as high quality, 14 as medium, and 18 as low. High-quality studies were primarily studies with clearly defined research objectives, justified sample sizes, validated measures for mental health problems, and transparent reporting of statistical methods. A detailed overview of study characteristics is provided in Appendix C.
Outcomes
The aim of this review was to synthesize evidence on the associations between SDOMH and mental health problems in youth with ID using a framework-led approach [27]. A great variety of SDOMH was found within the studies, which led us to categorize them into subdomains within our four main domains. Moreover, we explored whether associations within each SDOMH domain varied across subgroups based on ID severity, child age, and type of mental health problems. Table 2 summarizes the strength of evidence for each SDOMH domain, excluding the neighborhood domain, which had only one study and could not be assessed.
Table 2 Summary of strength of evidence per domainAssociations across subgroups of ID severity, age and type of mental health problem
To examine potential patterns within subgroups, studies were categorized based on ID severity, including individual levels (severe, moderate, mild, and borderline) as well as combined severity categories. Table 3 in Appendix F provides an overview of studies across these ID severity levels within each domain. This table presents the number of studies for each level or combination of ID severity across domains, indicating how many reported at least one significant result. Studies were fairly distributed across severity levels, with the social/cultural domain most consistently examined and yielding the highest proportion of significant findings. However, no consistent pattern of significant associations between SDOMH and mental health problems emerged across domains, indicating that specific domains were neither more frequently studied nor more strongly associated with mental health issues in any ID severity group.
Studies were then grouped based on age categories, including individual stages (early childhood [0–6 years], middle childhood [6–12 years], early adolescence [12–16 years], and late adolescence [16 + years]) as well as combined age groups. As shown in Table 4 of Appendix F, similar to findings by ID severity, there was no clear indication that specific domains are either more frequently studied or more closely linked to mental health issues across different age groups.
Finally, due to substantial variability in types of mental health problems reported and the absence of specified mental health conditions in some studies, conducting subgroup analyses for all mental health conditions was not feasible. We therefore focused on the two most frequently reported outcome groups—ASD and externalizing problems—based on a subset of 41 articles. Externalizing problems included studies reporting on outward-directed behaviors such as aggression, hyperactivity, conduct issues, and general behavioral problems. These conceptually similar constructs were grouped together to allow for meaningful comparison. As shown in Table 5 of Appendix F, the social/cultural domain was again the most frequently studied and showed the highest proportion of significant associations for both ASD and externalizing problems. However, the proportion of significant findings was greater for externalizing problems than for ASD within this domain. A similar trend was observed in the economic domain, despite the smaller number of studies overall. In contrast, ASD showed more significant associations in the demographic domain, relative to externalizing problems.
Domain 1. Demographic
The demographic domain included SDOMH reflecting general population characteristics, which were divided into two distinct subdomains: parental ethnicity and parental age. A total of eight studies examined these factors.
Parental ethnicity
Five studies examined associations between parental ethnicity and mental health problems in children with ID, including four cross-sectional and one longitudinal. The findings were mixed. Among the four cross-sectional studies, one reported significant differences in maternal race/ethnicity between children with ID only (higher proportion of non-Hispanic black mothers) and those with both ID and ASD [28]. However, three other studies reported no association between ethnicity and problem behaviour in children with ID [29,30,31]. Additionally, one longitudinal study focused on maternal migration rather than ethnicity directly, finding that children born earlier than four years before maternal migration were less likely to have ID with autism compared to those born in the year following maternal migration [32].
Parental age
Four cross-sectional studies examined the relationship between parental age and mental health problems in children with ID, though findings were inconsistent. One study found that mothers of children with both ID and ASD were significantly younger than those of children with ID only [28]. Another reported no age differences [33], while a third found that maternal age was not associated with emotional or conduct problems, but that older maternal age was linked to more hyperactivity [34]. A fourth study found no association between parental age under 18 and behavior problems in young children with developmental delays [35].
Domain 2. Economic
Within the economic domain, seventeen studies examined the role of economic factors in relation to mental health problems in children with ID. To synthesize the results, the economic factors were categorized into three subdomains: family income, income-related factors, and composite SES measures.
Family income
Four cross-sectional and two longitudinal studies examined a direct relationship between family income and mental health problems in children with ID, yielding inconsistent results. Whereas three cross-sectional studies reported no link between family income and mental health issues [36,37,38], one cross-sectional study found that children with ID from lower-income households were more likely to have psychiatric disorders [39]. Longitudinally, one study found no link [40], whereas the other study reported slower income growth over eight years in families of children with both ID and ASD compared to families with children who have only ID [41].
Income related factors
Six studies–five cross-sectional and one longitudinal–examined income-related factors and mental health in children with ID, with mixed results. Cross-sectional evidence indicated that household poverty was significantly associated with increased behavioral problems in children with ID [42]. Consistently, another study found that mothers of children with severe ID and behavior problems felt a greater need for financial help [43]. However, three studies found no significant associations between income-related factors, such as rented accommodation or reliance on benefits [44], Family Affluence Scale scores [45], and health insurance coverage [46], and mental health problems in children with ID. The longitudinal study found that over eight years, families with children with ID and ASD paid significantly lower federal taxes than those with only ID [41].
Composite SES measures
Six cross-sectional studies investigated composite SES measures, including financial hardship and socio-economic position. Remarkably, half of these studies did not specify how SES was measured. The results were either inconsistent or contradictory. In one UK study low socio-economic position, measured by household income, occupational prestige, and maternal education, was associated with more behavior problems in children with developmental delays [35]. Similarly, in another sample, lower SES (i.e., unspecified measures) was associated with increased behavior problems in children with ID [47]. In contrast, another study found that families of children with only ID had significantly lower SES compared to those with both ID and ASD, based on education level, occupation, employment status, and total household income [48]. Contrastingly, three studies found no significant link between SES and mental health problems in children with ID [49,50,51].
Domain 3. Social/Cultural
The social/cultural domain covers the broadest range of factors related to the mental health of children with ID. These factors are grouped into five subdomains: parental well-being, employment and education level, parent–child relationship, family dynamics, and life events. A total of 46 studies explored these associations.
Parental well-being
Parental well-being was reported in 23 studies, encompassing six different subcategories of well-being: general mental health, (di)stress, internalizing problems, substance use, maternal somatization and maternal life satisfaction. Each subcategory yielded results that were either mixed or inconsistent.
Ten studies, including eight cross-sectional and two longitudinal, examined the association between parental mental health and the mental health of children with ID. Cross-sectionally, six studies reported a link between lower parental mental health and increased psychological problems in children [31, 35, 39, 51,52,53]. Caregiver mental health problems were associated with higher rates of psychiatric diagnoses in children [39, 53], particularly in boys [29], and to increased depression and severe behavioral issues [51, 52]. Contrastingly, two studies found no significant difference in parental mental health between parents of children with and without behavioral problems [54, 55]. Longitudinally, both studies found that parental mental health problems were linked to increased psychopathology in children with ID one year later. One study associated parental mental health treatment history with variations in internalizing and externalizing problems [56], whereas the other found that parental mental health issues predicted psychiatric disorders in children [29].
Ten studies–five cross-sectional and five longitudinal–consistently linked greater parental (di)stress to increased behavior problems in children with ID, with seven focusing on maternal distress [42, 57,58,59,60,61,62]. Cross-sectionally, all five studies found at least one significant association between greater parental distress and increased child behavior problems [42, 58, 59, 61, 62], though links with having ASD were not significant [62]. Longitudinally, all five studies found a bidirectional relationship between parental distress and child behavior problems over time [57, 60], particularly for children's externalizing problems [56, 63, 64]. However, some associations, such as overall psychopathology [56], were not significant.
Eight studies investigated parental internalizing problems, encompassing depression (n = 7), anxiety (n = 3), and general internalizing problems (n = 1). Among the seven studies on parental depression, five were cross-sectional and two were longitudinal. Cross-sectionally, three studies found that higher maternal depression was associated with increased mental health problems in children with ID, specifically ASD [36], child depression [52], and maladaptive behavior [59], whereas two studies reported no significant link with behavioral problems [31, 54]. Longitudinally, one study found that higher maternal depression levels predicted increased internalizing and externalizing problems in children over time [65], whereas another study reported no association with internalizing problems [64]. Of the three studies on parental anxiety, two were cross-sectional, both showing that higher anxiety in parents was linked to more behavioral or psychiatric issues in children with ID [31, 36], whereas the longitudinal study found no significant link with internalizing or externalizing problems [64]. Regarding general parental internalizing problems, one cross-sectional study found no association with FX syndrome and autism but linked higher maternal internalizing symptoms to behavioral problems in adolescents and adults with FX syndrome [37].
Parental substance use was examined in two cross-sectional studies. One found that parental addiction was linked to increased externalizing symptoms in children with ID [66], whereas the other found no link between parental alcohol or drug abuse and behavior problems in children with developmental delay [35].
Two studies linked higher maternal somatization to increased behavioral problems in children with ID. A cross-sectional study found this among Latina caregivers of children with maladaptive behavior [59], whereas a longitudinal study identified maternal somatization as a significant predictor of increased behavioral problems over two years, particularly in mothers of children with both ID and ASD [57].
Maternal life satisfaction was examined in two studies. One cross-sectional study found no link with behavioral problems in children with ID [42]. A longitudinal study similarly reported no association over an eight-year period [63].
Employment and education level
Employment and education levels were reported in 19 studies, divided into four subcategories: child employment, parental employment, parental education, and a combination of parental employment and education. The findings within each subcategory were mixed, inconsistent or contradictory.
One longitudinal study explored employment among young adults with ID and found that those in open employment for two years had a decline in behavior problems, whereas those in training, sheltered employment or day recreation programs, showed no change [67].
Nine studies examined parental employment and child mental health, comprising seven cross-sectional and two longitudinal. Among the cross-sectional studies, two found that unemployment or lower job status correlated with more child behavior issues [39, 49] and ASD [49]. Consistently, children with ID from lower social classes were more likely to have conduct disorders, ADHD, and autism [39]. Inconsistently, three studies found no link between maternal employment and child behavior problems [30,

Comments (0)