
Remember me
This study explores the potential effects of LD comorbidity on screen-based device usage patterns. While there are similarities between the groups in some assessment categories, we believe that several differences warrant further examination. Before delving into the discussion of screen-based behaviors, it is important to address a notable issue regarding self-reported academic performance. Although the ADHD + LD group initially appeared to report lower academic achievement, this difference was not statistically significant when evaluated using adjusted p-values (p = 0.09). While it would be expected for the ADHD + LD group to show lower academic performance, this anticipated difference may have been influenced by several factors—such as defensive response tendencies, the inherent limitations of self-reported data, or discrepancies between perceived and actual academic functioning. As comparing academic performance between groups was not a primary focus of this study and was assessed only as a supplementary variable, we did not collect objective academic performance measures in a way that would allow direct comparison between groups. Nonetheless, it is worth noting that the two groups did differ significantly in terms of grade retention history, which may serve as a relatively more objective indicator of academic challenges and appears consistent with expectations regarding the ADHD + LD group. Therefore, we were unable to verify this finding through independent data, and it should be interpreted with caution.
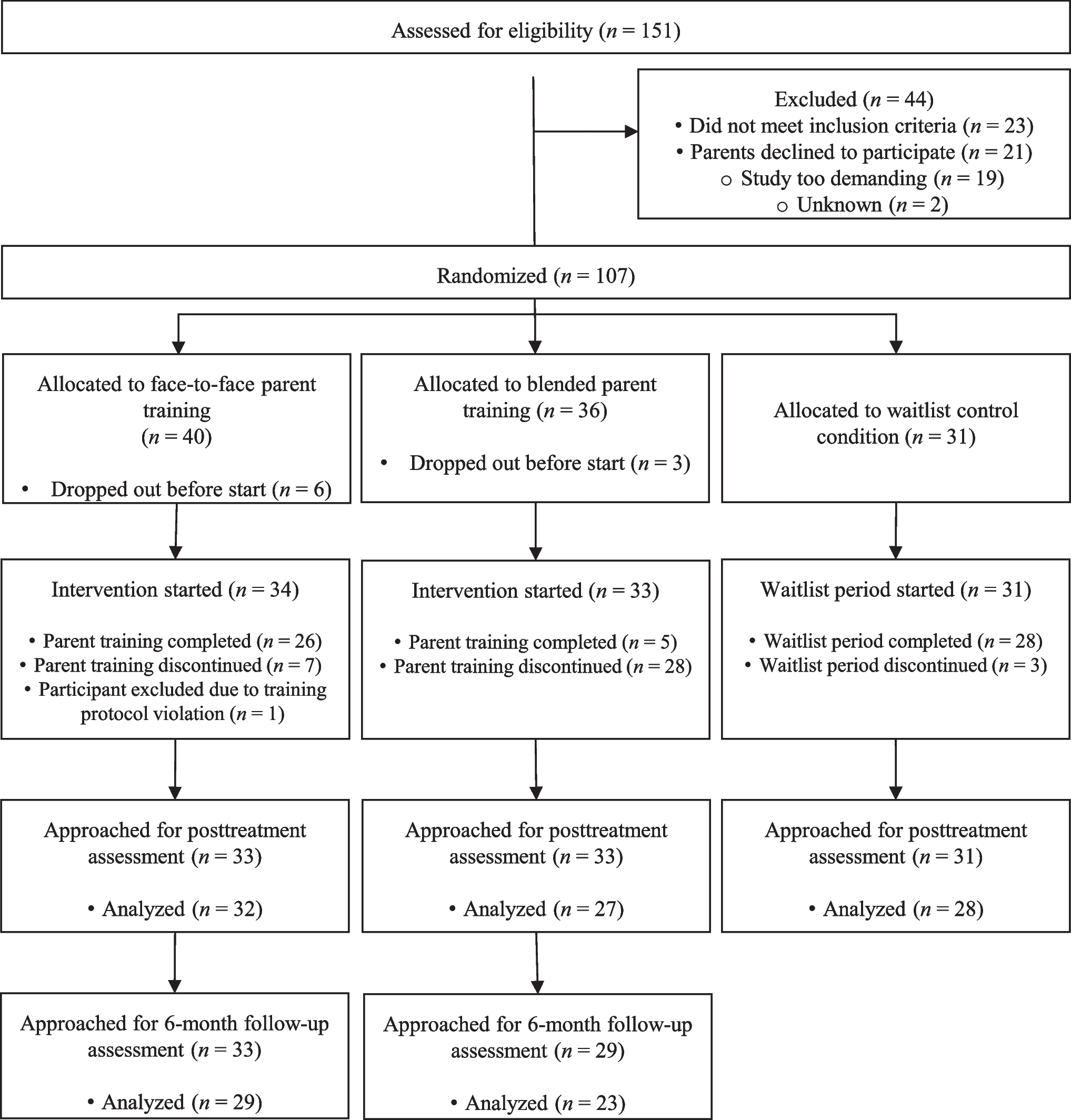
Fig. 1
Bar plot illustrating the proportion of adolescents in the ADHD-only and ADHD + LD groups who reported engagement in specific screen-based behaviors. The figure summarizes only those activities for which statistically significant group differences were found in the statistical analyses. The total number of devices used, although statistically different between groups, was not included due to scale-related visualization constraints
Our findings indicate that, for the ADHD + LD group, while there is no difference in daily screen time, there are differences in the usage patterns, compared to the ADHD-only group.
In terms of device usage, the ADHD + LD group was less likely to use PCs. Considering that groups were sociodemographically and financially similar, this result is most likely explained with youth preferences, rather than parents’ financial providing capabilities. Computers are more complex devices to learn and use compared to their alternatives, partly due to their more intricate user interfaces, and this is one possible reason why youth with LD may be less likely to use PCs [27, 28].
The ADHD-only group was also more inclined to use mobile phones and showed higher rates of usage for chatting, listening to music, watching movies/videos and engaging in educational activities.
It is undeniable that texting and chatting are the crucial parts of our daily lives. Today, there are many types of tablets on the market, with accompanying SIM cards and mobile internet connectivity, offering functions quite similar to those of mobile phones. However, mobile phones are more portable for daily use compared to the tablets, and the advantage on accessibility may explain the preference over tablets. From this perspective, it is understandable that the ADHD-only group, with higher texting rates, may tend to prefer mobile phones compared to the ADHD + LD group.
There are numerous digital applications and programs designed to assist youth with LD worldwide. Although widely used abroad, their use is limited in our country. On the other hand, there are numerous channels on social media platforms like Youtube and Instagram, creating contents aimed to help youth with formal education curriculum. However, considering that the target audience of those channels are healthy youth, the contents of those channels may be difficult to follow for youth with LD. This could explain why the technology use for educational purposes, which is expected higher in the ADHD + LD group, was found more frequent in the ADHD-only group. To conclude, it can be deduced that the ADHD + LD group tends to have fewer varied activities involving screen usage, while the ADHD-only group demonstrates more sophisticated and task-oriented screen use for various purposes.
Gaming and social media usage rates were similar between two groups. However, our study found those in the ADHD + LD are less prone to play MOBA, RTS and Puzzle & Platform game subgroups.
RTS is a term used to describe game types, where the goal is to dominate the opponent through resource management [29]. Age of Empires, Starcraft and Warcraft are well-known examples of the genre.
MOBA, which can also be defined as an RTS subgenre, refers to the games where each player controls a single character on a corridor with specific abilities, using resources to enhance their character’s certain abilities based on their teammates’ and opponents’ characteristics [30]. League of Legends, Defense of the Ancients, Heroes of the Storm, Brawl Stars are games that can be classified under this group.
Puzzle & Platform games, as the name suggests, are games where obstacles and puzzles must be overcome in order to progress. The range of this game group is broader compared to the aforementioned two subgroups, as both a 2D linear mobile game and a complex PC game like Portal are considered members of this group. Moreover, although not originally classified as puzzle games, horror/survival games like Amnesia and Outlast requires significant puzzle-solving skills, where next step is not explained and the players are pushed to find solutions under time pressure, to progress to the next level.
Evaluating these game subtypes within the context of the aforementioned knowledge, those game genres may require certain skills related to executive functions to succeed [31]. For example, in League of Legends, when the opponents have retreated to their center, in their absence, the player has limited time window to contest resources controlled by the opponents and gain an advantage. However, while doing that, the players need to calculate how long it will take for the opponents to return, monitor other lanes to ensure that all other opponents are in their lanes, as they may leave from time to time and gank (execute a coordinated attack to overwhelm the player) them. Moreover, the players need to stay alert all the time to actively track opponents’ skills and abilities’ cooldowns to decide when to attack, or when to retreat. When engaging the opponent, or when the players are being engaged, they need to react fast, counteract if possible, and shift focus to different targets for better outcomes.
There are studies suggesting that comorbidity with LD has a negative impact on executive functions in youth with ADHD; they have been found to exhibit weaker working memory and task-switching abilities compared to youth without LD comorbidity [32]. Additionally, youth with LD also demonstrate lower levels of coordination skills [33]. Moreover, gaming, especially RTS and MOBA subtypes, require teamplay and constant need of communication. Although voice chat is a more efficient option, the majority of communication in games is still occurs through text-based messsaging. That requires certain level of typing and reading skills which can be tough for youth with LD, especially for dyslexia subgroup. In light of this information, it can be speculated that youth with LD may find those game subtypes more challenging to play, and prefer these subgenres less, compared to their peers.
The results of our research also revealed that although there is no correlation between screen time per day and number of screen-based devices accessible to youth, there is a positive correlation between screen time per day and number of screen-based devices owned by youth. To the extent of our database searches, we did not find any other research examining the duration of screen-based device ownership, number of screen-based devices owned by youth and number of screen-based devices accessible to youth and their correlation between screen time per day. To our knowledge, our research is the first study in the literature evaluating the relationship between these three parameters and screen time per day.
The finding that, number of devices owned by youth shows positive correlation while number of devices accessible to youth showing no correlation at all can be explained by the indirect limiting effect on the availability of devices for youth’s use. Devices owned by parents or shared with siblings are not always available for youth. Conversely, when the devices are not occupied, the youth may be busy with daily tasks and other activities, thus limiting time spent on screen. As expected, when the youth have their own devices, they have more opportunities to use it for the same reasons; as the number of devices owned by youth increases, so does screen time, since they have more options to turn to.
On this matter, limiting screen-based device ownership may be more challenging in practice than it might seem. Youth require PCs or tablets to use for their homework. It is also understandable that parents’ concern for their children’s needs and well-being, and being able to contact them in times of need. Therefore, many parents buy their children mobile phones and although it is bought with good intentions, the unintended consequences cause the problem. Under these circumstances, especially for smaller children, who are less likely to regulate themselves on time spent on screen, smartwatches with SIM card functionality might offer a better alternative, which are similar to mobile phones in terms of communication capabilities, and less likely to be overused by youth due to limited features.
Our results showed a correlation between the increase in the duration of ownership of a screen-based device and screen time per day. Neuroimaging studies show certain alterations in the reward circuits of the brain in the individuals with IGD, just like other addictions [19]. Cognitive Behavioral Approach also theorizes that gaming behavior, as a source of pleasure, creates a self-reinforcing cycle [34]. Combining these insights with the previously discussed negative effects of owning a screen-based device, such a result is not surprising.
IGD is a diagnosis with a well-known comorbidity of ADHD. It’s thought that impulsivity and self-regulation difficulties in ADHD play a role in IGD etiopathogenesis. This theory led to treating IGD with ADHD pharmacotherapy, which led to beneficial results [35]. Another study demonstrated improved outcomes in treating IGD patients with Methylphenidate over a 3- month follow-up period, compared to the control group [36]. Our results indicate no correlation between methylphenidate treatment duration and screen time per day. Since the primary aim of our study to examine the possible effects of LD comorbidity on youth with PTU, the participants were recruited from patients who had been receiving methylphenidate treatment with at least 6 months, to eliminate potential confounding factors. Therefore, it can be deduced that the majority of the benefits of methylphenidate treatment on IGD comorbidity emerge within 6 months of the treatment, while the following period primarily contributes on maintaining the achieved outcomes.
Our results also show that youth who have imposed limits on screen time tend to be younger, spend less time on screens, and engage less frequently in social media and chatting. Younger children, who are more likely to comply with parental authority, are easier for parents to manage in terms of limiting screen time, as expected. It’s also understandable that younger children prefer to spend less time on these activities, because they are more adolescent and adult-oriented activities. We might speculate that, these younger children could also be interested in these activities; however, they prefer to spend their limited and valuable screen time playing games; which is expected to be the most pleasurable activity for them.
While the overall levels of problematic technology use did not differ significantly between groups, the differences observed in usage patterns may still carry clinical relevance. Rather than focusing solely on the duration of screen use, clinicians might benefit from considering what purposes screen time serves for each individual. For instance, if a child’s engagement with technology is partly shaped by the relative difficulty they experience with academic tasks, rather than being driven by impulsivity, it may point to different underlying needs and require distinct clinical considerations. Furthermore, exploring what children do during screen time, such as the type of content they engage with or the devices they prefer, may offer indirect clues about potential comorbidities. A child who consistently avoids cognitively demanding games or prefers simpler interfaces, such as tablets instead of computers, might be exhibiting signs related to underlying learning difficulties. Thus, assessing usage patterns in more detail could support a more nuanced understanding of the child’s functional profile.
LimitationsOur study is among the first to investigate the relationship between PTU and LD in ADHD-diagnosed children. However, it is not without limitations. Being a single-center study represents a limitation regarding the generalizability of our findings. Additionally, the relatively small sample size may have limited the statistical power of our analyses and prevented more detailed subgroup evaluations—particularly in relation to participant-level characteristics such as age and gender, which could offer further insights given that technology use preferences may vary across these dimensions.
Furthermore, as our study was cross-sectional in design, causal inferences could not be established. Rehabilitative educational approaches for LD may have an effect on the relationship between PTU and LD. Nevertheless, due to the variability in the types and durations of educational modules provided by different institutions, standardization could not be achieved, and this factor was excluded from the study.
We did not have the opportunity to evaluate thoroughly the hardware specifications of the devices used by youth. Considering that high-performance devices may offer more options, particularly in the gaming domain, we believe, this may be also a potential limiting factor of our study.
Comments (0)