
Remember me

Pericarditis is a major cardiac manifestation associated with autoimmune disorders. In 1882, Charcot described pericardial disease in patients with rheumatoid arthritis. Moreover, pericardial involvement extends to other auto-immune disorders such as systemic lupus erythematosus (SLE), Sjogren’s syndrome, systemic sclerosis, and vasculitis, in addition to organ-specific diseases such as inflammatory bowel disease [1,2,3]. The clinical spectrum of pericardial involvement in autoimmune disorders includes acute, recurrent, incessant, chronic pericarditis and constrictive pericarditis, asymptomatic pericardial effusion, and rarely cardiac tamponade [4]. In some cases, pericardial symptoms herald the presentation of disease, in the absence of other systemic manifestations. Over the past decade, there has been a resurgence of interest in further understanding pericardial disease secondary to autoimmune conditions. There is a clear distinction between the pathophysiology of autoinflammatory and autoimmune conditions, which is reflective of the presentation and prognosis. The aim of this review is to explore the state-of-the-art diagnostics and therapeutics in the management of autoimmune pericarditis (AAP).
EpidemiologyAcute pericarditis regardless of the etiology represents 5% of patients presenting to the Emergency Department with chest pain. However, the true incidence of pericarditis varies based on the population. The annualized prevalence estimate is 48 patients per 100,000 persons in the U.S [5], compared to a reported estimate of 27.7 cases per 100,000 person years in an urban area in Northern Italy [6]. The overall incidence rate of acute pericarditis increases with age; the ages of patients with acute pericarditis in clinical series have ranged from 33 to 73 years, with a median age of 56 years [7, 8]. The role of gender in acute pericarditis has varied between murine experimental studies and clinical studies with a male/female ratio of 1.42 in some studies [9, 10]. A rheumatic etiology is present in 2–7% of patients with acute pericarditis and around 10% of recurrent pericarditis. Rheumatologic diseases manifesting in pericarditis have been classified immunologically as autoimmune and autoinflammatory.
The following review will focus on autoimmune conditions that are commonly associated with pericarditis, such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis, Sjogren’s syndrome and vasculitis. The clinical diagnosis of pericarditis is largely based on symptoms. However, the true incidence may be underreported due to asymptomatic cases. For instance, asymptomatic pericardial disease has been identified in more than 50% of SLE patients [11]. Furthermore, the reported rising prevalence of both clinical and subclinical autoimmune conditions may potentially reflect an increase in pericardial conditions [12].
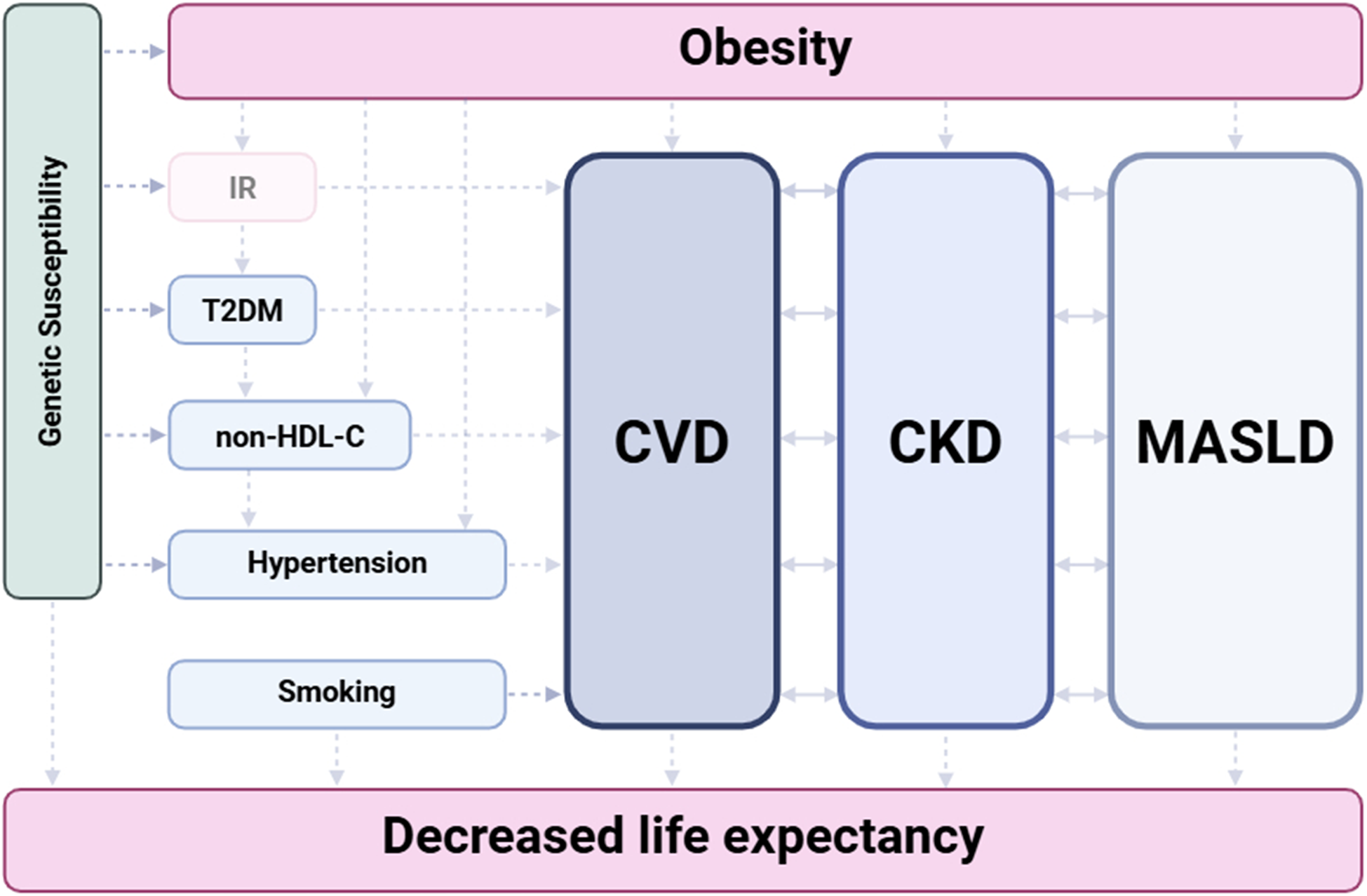
PathophysiologyAcute pericarditis is a heterogeneous condition characterized by inflammation of the pericardium. The pathophysiology involves an inflammatory response, typically mediated by the innate immune system, with neutrophils and macrophages playing significant roles. Some authors have classified acute pericarditis into two distinct sub types: autoimmune and autoinflammatory. The extent of involvement of the innate and adaptive immunity is based on the subtype. Interleukin-1 and NACHT, leucine-rich repeat, and pyrin domain-containing protein (NLRP3) play a central role in idiopathic recurrent pericarditis and autoinflammatory conditions, while in autoimmune disease such as SLE, there is a predominance of type 1 interferon signature [13, 14]. Even so, not all patients with SLE have the interferon signature [15] (Fig. 1; Table 1).
Fig. 1
Pathophysiology for autoimmune pericarditis. The asterisk (*) signifies the mutation which is also shown on the Act1 receptor with the little orange piece. Act1: Act1 adaptor protein, essential intermediate for IL-17; C3: complement component 3; IFN: interferon; IL: interleukin; TNF: tumor necrosis factor; TRAF3IP2: TRAF3 interacting protein 2
Table 1 Comparison of pathophysiology and presentation of autoimmune diseases associated with pericarditisSimilar to acute pericarditis, the pathophysiology of recurrent pericarditis (RP) is complex and involves both autoimmune and autoinflammatory mechanisms. Autoimmune contributions are suggested by the presence of autoantibodies and associations with rheumatologic disorders, such as SLE. Autoinflammatory mechanisms are primarily driven by the activation of the inflammasome, particularly the NLRP3 inflammasome, leading to the production of interleukin-1 (IL-1) and similarities with autoinflammatory condition such as Familial Mediterranean Fever (FMF) [16]. The degree of predominance of either mechanism led to the suggestion by Tombettti et al. to stratify patients with recurrent pericarditis into three phenotypes [17]:
a) An autoimmune type, highlighted by features occurring in systemic autoimmune diseases (e.g., arthralgias, dry eyes, Raynaud’s phenomenon), moderate C-reactive protein (CRP) elevation, frequent autoantibody positivity (anti-nuclear antibodies (ANA), anti-heart antibodies (AHA) and anti-intercalated disk autoantibodies (AIDA). This subtype shares the hallmarks seen in autoimmune disorders. Anti-nuclear antibodies are a frequent finding in patients having RA, with a prevalence up to 45% compared to 15% of healthy patients [18]. Anti-heart autoantibodies and anti-intercalated disk autoantibodies are present in about 67.5% of patients with RP [19]. The production of such autoantibodies may be due to the above-mentioned processes, where the exposition of autoantigens could stimulate an immune response and the activation of T and B lymphocytes. Alternatively, these autoantibodies may simply be biomarkers without a pathogenic role [20]. This is likely the dominant phenotype in autoimmune disorders, although overlap is present.
b) An autoinflammatory phenotype, highlighted by recurrent relapses followed by complete resolution, symptomatic serositis, high fever associated with high CRP and absence of autoantibodies, with major clinical similarities to autoinflammatory disease such as Familial Mediterranean Fever (FMF), or tumor necrosis factor receptor-associated periodic syndrome (TRAPS). It has been suggested that some of these patients might have an atypical or subclinical form of an autoinflammatory disease, e.g., genetic disorders characterized by primary dysfunction of the innate immune system and caused by mutations of genes involved in the inflammatory response.
c) A nonspecific phenotype, characterized by mildly symptomatic patients with few attacks, subacute course, smoldering elevation of inflammatory markers, and no evidence of autoimmunity [17].
It is not fully understood how much innate and adaptive immunity contributes to the immunopathogenesis of pericarditis in the setting of autoimmune disease; limited research exists exploring pathophysiological mechanisms that drive the heterogeneity of outcomes observed in specific forms [16, 21]. In the following section, the pathophysiology of pericarditis will be addressed according to specific auto-immune diseases that are the most known to be associated with pericarditis:
Systemic Lupus Erythematous (SLE)Acute or chronic inflammation of the pericardium in SLE are mostly thought to be triggered by C3 deposition in the pericardial tissue [22]. Genetic variability coding for innate and adaptive immunity affects the disease phenotype and the risk of pericarditis. A study by Perricone et al. concluded that single nucleotide polymorphism in the TRAF3IP2 gene that codes for Act1 (a signaling receptor in IL-17 mediated immune processes) was associated with higher risk for pericarditis in SLE patients [23].
Rheumatoid ArthritisAlthough scant literature exists on the pathophysiology of pericarditis in RA, it is usually present in patients with a positive rheumatoid factor (RF). Furthermore, it has been shown that cytokines involved in the inflammatory process of RA (IL-1, IL-6, TNF-α) are also involved in cardiac manifestations of RA including pericarditis [24].
Systemic SclerosisFluid analyses from pericardial samples in patients with scleroderma were found to be predominantly exudative. In contrast to other auto-immune diseases, there was lack of auto-immune activity, such as autoantibodies, immune complexes and complement deposits [25, 26]. Lefèvre et al. reported a prevalence of 30% of pericardial effusion in patients suffering from systemic sclerosis (SSc)-associated pulmonary hypertension (PAH). As pericardial effusion is often associated with immunological disease even without a diagnosis of PAH, this difference is probably due to the heterogeneity of the causes and the severity of pulmonary hypertension [27].
Primary Sjogren Syndrome (SS)Sjogren’s syndrome is a chronic inflammatory condition associated with lymphocytic infiltration of glandular and extraglandular organs. Though numerous cytokines (IFN and IL17/IL23) and B cells play a pivotal role in the pathogenesis of SS, their role in associated pericarditis is not well defined [28].
VasculitisPericardial involvement is rare when compared to other cardiac manifestations (myocarditis, coronary disease, aortic disease) in small-, mid- and large-vessel vasculitis [29]. Although the exact pathway of pericardial inflammation is still unclear, the similar response of both pericarditis and vasculitis proves a common pathogenesis [30, 31]. The chronic exposure of vasculitis patients to immunosuppressive medications could also increase the risk of exposure to viral infections, which could in turn lead to acute or recurrent pericarditis [31].
Clinical Presentation (Fig. 2; Table 1)Fig. 2
Pericarditis presentation and diagnosis
The clinical presentation of AAP in general is associated with acute inflammatory response and rarely is the initial presenting feature of the disease [32]. A recent study of 471 patients, of which 7% were noted to have autoimmune disease, described in detail the variation of presentation in patients under the age of 75 years compared to over 75 years (geriatric group). Younger patients presented more frequently with chest pain, pericardial rubs, widespread ST- segment elevation, while the geriatric group depicted more commonly dyspnea, pericardial and pleural effusion [8].
SLE and PericarditisPericarditis affects up to 50% of patients and is usually mild and rarely compromises the patients hemodynamically [22]. Pericarditis can present at onset of SLE or as part of a recurrent flare or isolated [33, 34]. There are few case reports where the initial presentation of acute pericarditis precedes the diagnosis in < 1% of patients [35, 36]. Even so, it is important to emphasize that most of the pericardial involvement in SLE is asymptomatic [37]. Factors associated with increased risk of pericardial involvement include male gender with active disease in conjunction to cytopenia, proteinuria, fever, lymphadenopathy, interstitial lung disease and Raynaud’s disease and lupus anticoagulant [38, 39].
Rheumatoid Arthritis and PericarditisSimilarly to SLE, pericarditis is the most frequent cardiac manifestation in RA with nearly 40% of pericardial involvement [40]. Symptomatic acute pericarditis is infrequent in RA (10% or less), while one out of three patients would have an incidental pericardial effusion on imaging. Acute presentation is usually associated with advanced disease and elevated biomarkers [41, 42]. Rare case reports display pericardial disease preceding diagnosis of RA [43]. Other pericardial manifestations seen in newly diagnosed and long-standing RA are cholesterol pericarditis and effusive-constrictive pericarditis [44]. Cholesterol pericarditis is a rare entity with chronic, large, cholesterol-rich pericardial effusions. Although the pathophysiology of this accumulation is unclear, the sources of cholesterol are thought to be blood and associated inflammation [45].
Systemic Sclerosis and PericarditisAutopsy studies have shown that ~ 70% of systemic sclerosis patients had chronic pericarditis or pericardial involvement, although only 5–20% eventually develop symptoms. Risk of pericardial disease is increased 8-fold compared to the general population and mostly related to pulmonary hypertension rather than acute pericarditis [46]. Clinically symptomatic pericardial effusions are present in only 5–16% of SSc patients and pericardial tamponade is rare (0.2%). However, hospitalized patients with cardiac tamponade had a significantly increased mortality rate of 17.7%, compared to 8.8% in patients with pericardial effusions without a tamponade physiology [47].
Sjogren’s and PericarditisPericardial involvement in Sjogren’s may often be asymptomatic and remains relatively rarely reported [48, 49]. Rare cases of either acute pericarditis or constrictive pericardial disease have been reported [48].
Vasculitis and PericarditisIn antineutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis (AAV), pleural and pericardial involvements are well recognized in eosinophilic granulomatosis with polyangiitis (EGPA) but considered rare manifestations of the other forms of AAV [3]. Giant cell arteritis (GCA), also known as temporal arteritis, is a vasculitis of large and medium-size vessels that involves the extracranial branches of the carotid artery and is of unknown etiology affecting adults age > 50 years. Cardiac manifestation is estimated to occur in about 5% of GCA patients. Pericardial involvement is rare and range from 1 - 3% [50, 51].
ComplicationsRecurrent PericarditisRecurrent pericarditis (RP) is associated with substantial morbidity. There is limited data for recurrent pericarditis in autoimmune disorders. A recent letter from a single institution reported 50% higher recurrence rates in AAP as compared to that of idiopathic pericarditis [52]. Younger age, moderate-severe late gadolinium enhancement and steroid use were associated with higher recurrence rates [52]. The timing of recurrence can be impacted by the disease entity such as in SLE, where it is likely to occur within one year of the onset of pericarditis.
Cardiac TamponadeA recent nationwide Japanese cohort of 20,000 hospitalized patients with pericarditis sought to investigate the rates of cardiac tamponade in AAP. There were 170 AAP, and 5,027 acute idiopathic pericarditis (AIP) patients identified. The rate of in-hospital death was not significantly different between the AIP pericarditis and AAP groups (73 of 5,027 [1.5%] vs. 3 of 170 [1.8%]; P = 0.75), whereas cardiac tamponade was significantly more common in patients with AAP than in those with AIP (237 of 5,027 [4.7%] vs. 15 of 170 [8.8%]; P = 0.023). Among patients with AAP, SLE was the most common diagnosis associated with cardiac tamponade complications, followed by rheumatoid arthritis and systemic sclerosis [53].
Constrictive PericarditisNeither the rates of constrictive pericarditis in autoimmune disorders nor the role of immunity and immunosuppressive agents in mitigating this risk are known. Further research is needed to address these gaps.
Diagnostic StudiesElectrocardiogram (EKG)Classic EKG findings include ST elevation and PR depression seen in 60% of patients with acute pericarditis, while up to 40% of patients present with atypical and non-diagnostic EKG findings [54].
Laboratory DataElevated biomarkers i.e., C-reactive protein (CRP) and estimated sedimentation rate (ESR) are the hallmark of diagnosis which may be associated with autoimmune disease activity. Pericardial fluid analysis may provide additional diagnosis value. For example, glucose level (< 45 mg/dL), elevated protein (> 5 g/dL) and leucocyte count (> 15,000/πL) may suggest RA as the underlying diagnosis. Other associated findings suggestive of RA are high pericardial RF and immunoglobulin G levels, with a low total serum hemolytic complement. In RA with nodules, cholesterol levels are seen to be elevated in the pericardial fluid. Therefore, if autoimmunity is suspected a detailed analysis of pericardial fluid may be key. In a cohort of 422 patients with recurrent pericarditis, (15% with autoimmune disease), there was a correlation of inflammatory markers such as ESR and hs-CRP (high sensitive CRP) with late gadolinium enhancement (LGE) on Cardiac MRI (CMR), which underscores that biomarkers maintain an important role in autoimmune pericarditis [55].
Imaging ModalitiesChest X-rayPlain chest radiographs (CXR) will often be normal in patients with acute pericarditis. Enlargement of the cardiac silhouette (cardiothoracic ratio (CTR) > 50%) on CXR has a moderate sensitivity (71%), but low specificity (41%). Logically, specificity increases as cardiomegaly increases (76% with CTR of 60%) [56]. In a study of 135 patients with confirmed constrictive pericarditis, pericardial calcification on CXR was present in 27% of cases. Thus, pericardial calcification is suggestive of constrictive pericarditis [57].
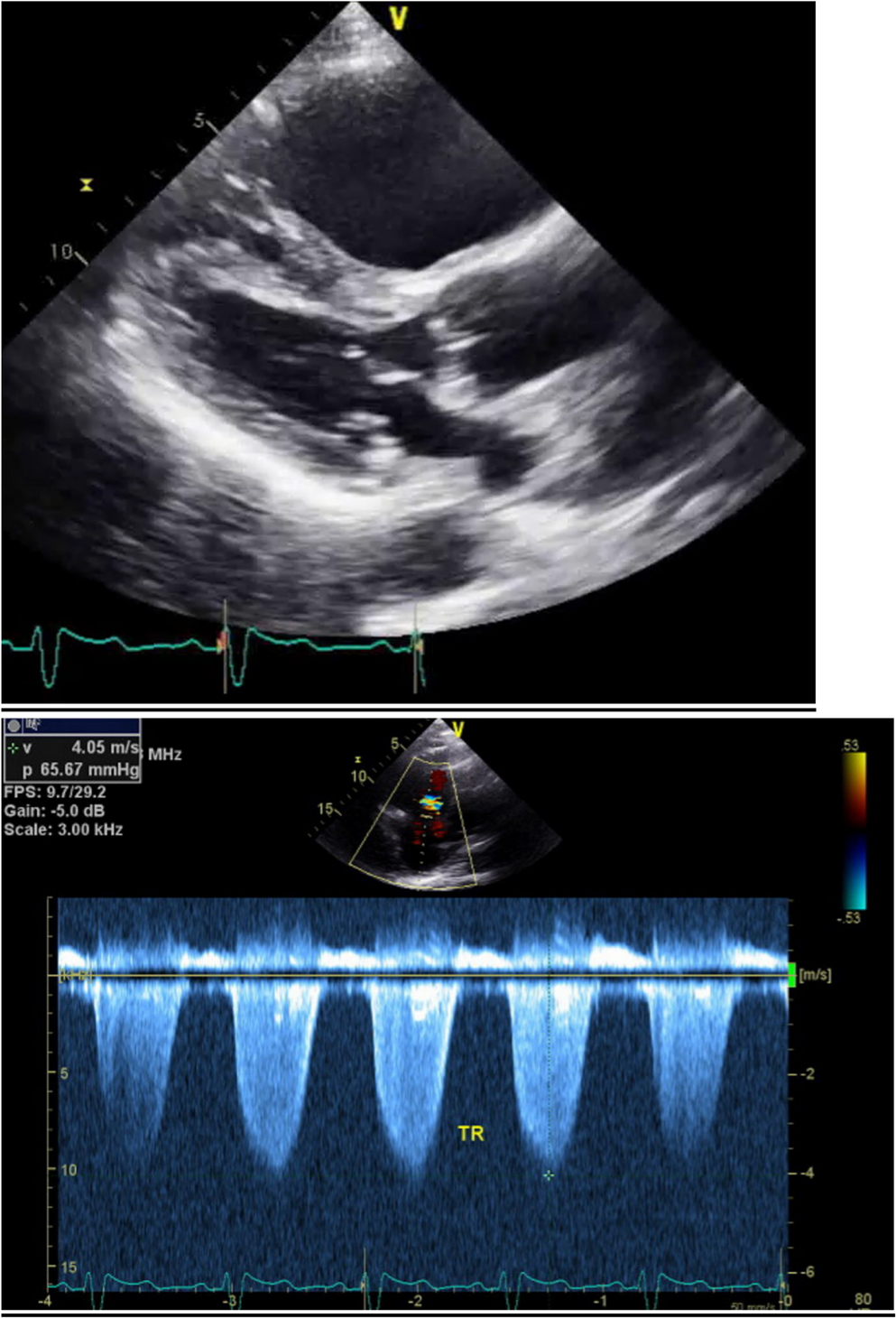
EchocardiographyTransthoracic echocardiography (TTE) remains the first line in diagnosis imaging of pericardial disease due to its widespread availability and low cost. Echo evaluation is key to determine the size of the effusion as well as the hallmarks of constrictive physiology. The size of the effusion is determined by the largest dimension of the echo-free space at end-diastole and stratified as such: trivial (only seen in systole), small < 1 cm, moderate 1–2 cm, large > 2 cm and very large > 2.5 cm [58, 59]. Transudative effusion compared to exudative effusions are determined by typical anechoic nature of the former compared to the heterogenous appearance of the later. Epicardial adipose tissue is increased in patients with autoimmune disorders [60] and may mimic pericardial effusion. Pericardial thickening is sometimes also seen in pericarditis.
Constrictive physiology involves two unique features:1) dissociation between intrathoracic and intracardiac pressure with respiration; and 2) interventricular dependance with increased diastolic filling pressure in both right- and left-sided chambers. This dynamic is translated to TTE parameters proposed as the Mayo Clinic Echocardiographic Diagnostic criteria for constrictive pericarditis, which include: a) E predominant mitral inflow with respiratory variation (E/A ratio > 0.8); b) dilated inferior vena cava usually with minimal collapse; c) Respiro-phasic ventricular septal shift caused by ventricular interdependence; d) elevated medial mitral early diastolic velocities (e’) > 8 cm/sec, often higher than compared to lateral e’ (also known as annulus reversus) and e) expiratory end diastolic hepatic venous flow reversal velocity/forward flow velocity > 0.8. The combination of respire-phasic ventricular shift and elevated medial e’ have a positive predictive value of 99% [58, 61]. Recent advances in 3D and strain suggest a role for this modality in the diagnosis of constrictive pericardial disease. Circumferential strain is more likely to be reduced in constriction compared to global longitudinal strain seen in autoimmune condition, such as SLE [62]. There is also a unique regional longitudinal strain pattern that has been demonstrated in constriction, in which the lateral ventricular strain is reduced as compared with the septal ventricular strain (also known as strain reverses). This is due to the tethering effects of the constrictive pericardium [63].
Cardiac CTCardiac CT has a supplementary and more limited role in the evaluation of pericardial disease. Pericardial thickening may be seen in pericarditis although chronicity cannot be determined, whereas pericardial calcifications can be seen in chronic constrictive pericarditis. Furthermore, cardiac CT can be used to assess pericardial effusion size and characterization can be assessed. CT also has an important role in the pre-operative planning for procedures such as pericardiocentesis and pericardiectomy [64].
Cardiac Magnetic Resonance (CMR)CMR offers a comprehensive second-line modality and has increasingly rendered its value in the diagnosis and management of pericardial disease. Current CMR protocols include steady-state free precession to evaluate chamber size and function, real-time free-breathing imaging critical for assessing respire-phasic septal shift, black blood spin echo sequence with and without contrast (T1 and T2 weighted inversion-recovery turbo spin echo sequences) to elicit pericardial anatomy and thickening, T2 short tau inversion recovery (STIR) to identify pericardial edema and late gadolinium enhancement (LGE) to identify pericardial inflammation and fibrosis [58, 65].
In the acute phase, there is typically increased signal in both T2-STIR and LGE. In the chronic phase, the former disappears, and the latter is correlated with severity and outcomes. In the recent protocol predefined substudy of the RHAPSODY trial, patients with moderate-severe LGE had a higher number of recurrences than patients with mild pericardial LGE [66]. Although CMR has cemented its role in management and prognosis of pericarditis, its widespread use is hindered by cost and institutional constraints.
18F-fluorodeoxyglucose-positron Emission Tomography/computed Tomography (18FDG-PET/CT)In past decades, the role of 18FDG-PET/CT has grown in identifying sources of inflammation, yet its role in pericardial disease remains unclear. In 2015, European Society of Cardiology guidelines recommended 18FDG-PET/CT in limited cases for the diagnosis of autoimmune (large-vessel arteritis) and autoinflammatory (sarcoidosis) conditions. For example, increased FDG uptake in multiple large vessels throughout the body may indicate a disease such as large-vessel vasculitis [67]. This modality can aid in the differential diagnosis of alternative etiologies for pericarditis. In one study of 107 patients, a maximum standardized uptake value (SUV max) ≥ 5 typically was associated with tuberculosis or neoplastic or autoimmune disease compared to < 5 in idiopathic pericarditis [68]. One of the major limitations of 18FDG-PET/CT in autoimmune disorders is the reduced sensitivity with the use of corticosteroids for diagnosing inflammation. This has been demonstrated in several diseases, including large-vessel vasculitis, rheumatoid arthritis, and polymyalgia rheumatic [69]. As such, it is recommended to delay the commencement of corticosteroid treatment until FDG-PET/CT is performed, unless there is a risk of severe complications such as ocular ischemia in temporal arteritis. 18FDG-PET/CT is an adjuvant tool where the etiology of pericarditis is unclear.
Treatment (Table 2)Table 2 Medications used in autoimmune pericarditis (administration, side effects, and efficacy)Acute and recurrent pericarditis has been reported in association with treatments such as corticosteroids, hydroxychloroquine, mycophenolic acid, cyclophosphamide, and azathioprine. As a result, a standard protocol previously suggested for idiopathic acute and recurrent pericarditis may be of limited utility [39]. The understanding and knowledge of available therapies is critical to tailor therapies effectively. First-line treatment for acute pericarditis includes non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or aspirin, combined with colchicine. Corticosteroids are considered as well depending on the severity of presentation, particularly for patients who do not respond to NSAIDs and colchicine or have contraindications to these medications. For refractory cases or those with multiple recurrences, interleukin-1 (IL-1) inhibitors such as anakinra and rilonacept have shown efficacy. Immunosuppressive agents like azathioprine and intravenous immunoglobulins (IVIG) may be considered in severe, refractory cases, when corticosteroids an
Comments (0)