
Remember me
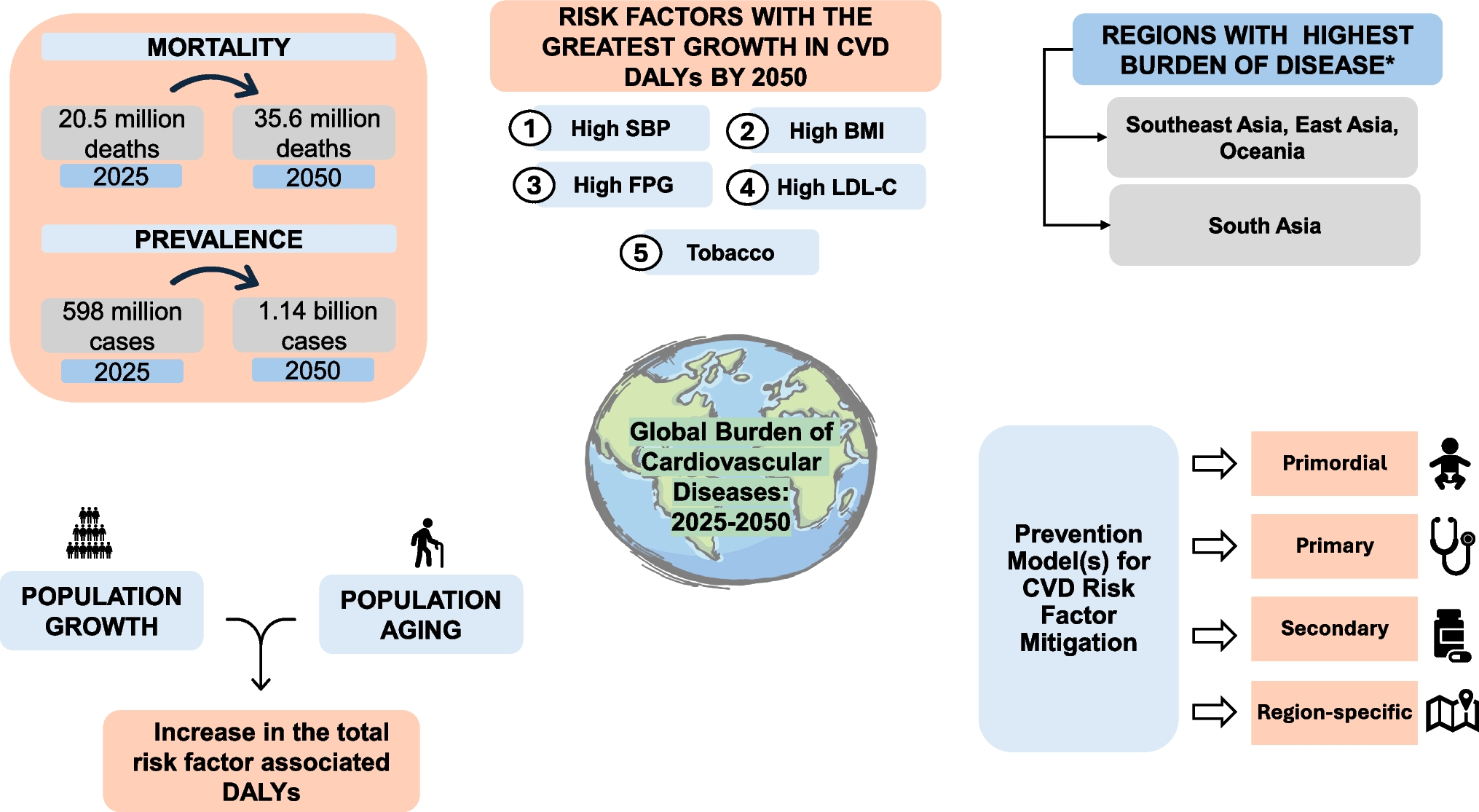

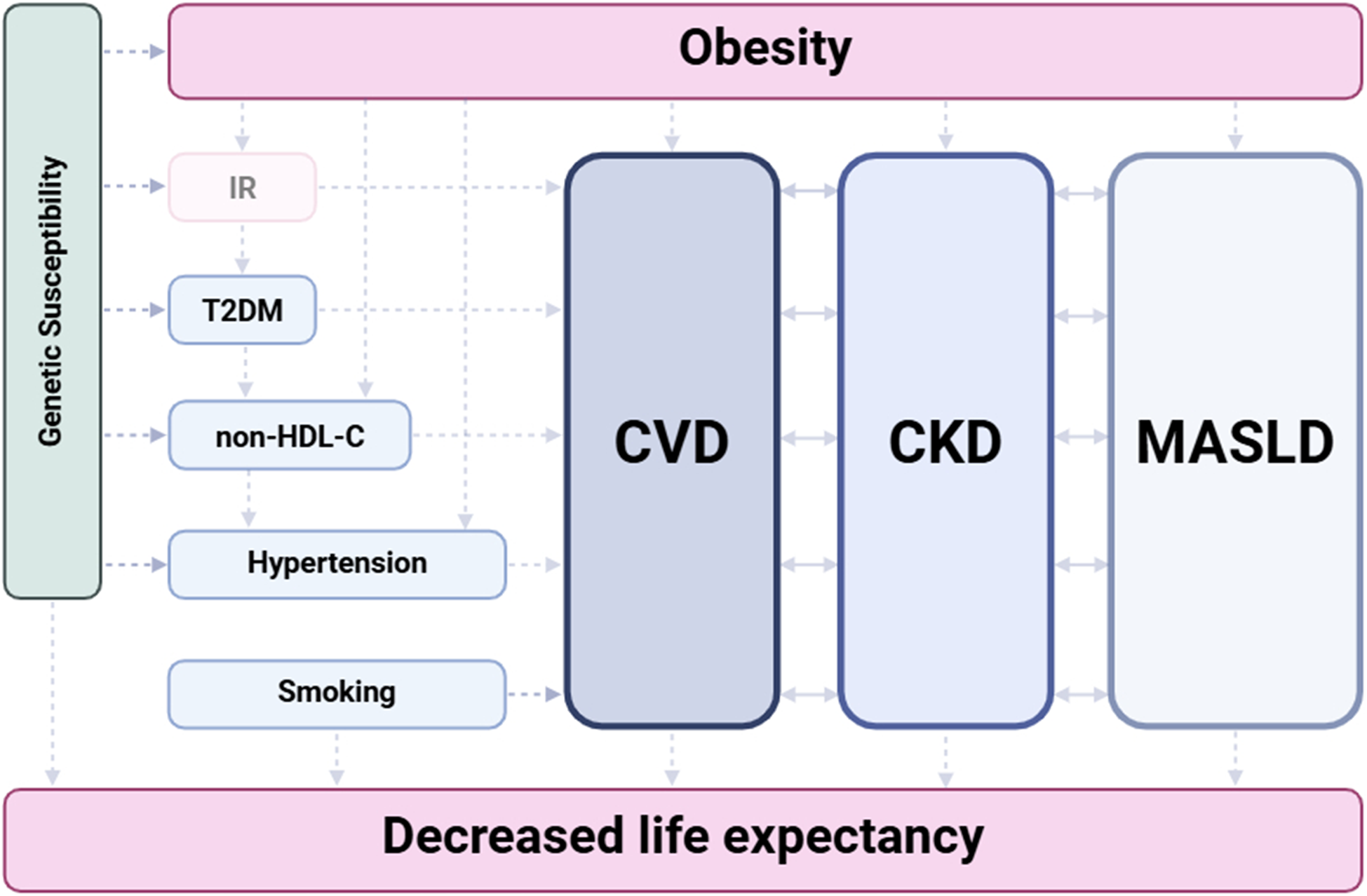
GLP-1 is an incretin hormone secreted by L-cells in the small intestine in response to nutrient ingestion. It enhances glucose-dependent insulin secretion, suppresses glucagon release, delays gastric emptying, and promotes satiety [16]. GLP-1 RAs are analogs or mimetics of endogenous GLP-1 that bind to the GLP-1 receptor on pancreatic β-cells and other tissues [17]. Beyond glycemic control, GLP-1 receptors are expressed in cardiovascular tissues, the central nervous system, and renal glomeruli. These agents exert pleiotropic effects, including anti-inflammatory and anti-atherogenic properties, modulation of blood pressure, and improvements in endothelial function. Renal benefits are believed to be mediated via reduction in albuminuria, tubular-glomerular feedback, and direct renal hemodynamic effects (Fig. 1). These mechanisms provide the biological plausibility for cardiorenal benefits observed in GLP-1 RA outcome trials [5, 7, 13].
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Overview of the physiological effects of GLP-1 receptor agonists across major organ systems. Abbreviations: GIT, gastrointestinal tract; GLP-1, glucagon-like peptide-1
Oral GLP-1 RAs: Innovation and Clinical RationaleSemaglutide is the first and only GLP-1 RA currently approved by the U.S. Food and Drug Administration and the European Medicines Agency for both subcutaneous and oral forms [18]. The development of oral semaglutide, a peptide-based GLP-1 RA co-formulated with sodium N-[8-(2-hydroxybenzoyl) amino] caprylate (SNAC), did overcome the challenge of peptide degradation in the gastrointestinal tract. This innovation allowed for the first oral formulation of a GLP-1 RA, offering a more convenient alternative to injectable agents while maintaining comparable efficacy in glycemic control. However, oral semaglutide requires strict administration conditions, including ingestion in a fasting state with a limited volume of water and a mandatory post-dose fasting interval, factors that may compromise adherence and real-world therapeutic effectiveness [13].
More recently, orforglipron, a non-peptide, small molecule GLP-1 RA, has emerged in clinical trials. Unlike oral semaglutide, orforglipron does not require special co-formulation strategies and bypasses the limitations of enzymatic degradation and poor absorption. This pharmacologic profile supports the potential for once-daily, food-independent dosing, offering greater convenience and the prospect of improved treatment adherence [19]. Early studies have shown promising glycemic control and weight loss outcomes, with large cardiovascular outcome trials are underway [19,20,21].
Randomized Controlled Trials (RCT) on Oral SemaglutidesPIONEER 6: Non-Inferiority Trial Evaluating CV Safety of Oral Semaglutide [13]The PIONEER 6 trial was a double-blind, placebo-controlled, randomized trial for CV outcomes evaluating the safety of oral semaglutide in patients with T2DM and high CV risk. There were 3,183 participants with CV or chronic kidney disease randomized to receive either oral semaglutide or placebo over a median follow up of 15.9 months [13]. The primary endpoint, a composite of MACE (CV death, nonfatal myocardial infarction (MI), or nonfatal stroke), occurred in 3.8% of the semaglutide group and 4.8% of the placebo group. While the difference was not statistically significant (hazard ratio, 0.79; 95% CI, 0.57–1.11, P < 0.001 for noninferiority), the study met criteria for non-inferiority. Notably, semaglutide was associated with a 51% relative risk reduction in CV death (HR, 0.49; 95% CI, 0.27–0.92), though this was a secondary outcome [13]. Although limited by its short duration and modest sample size, PIONEER 6 confirmed the CV safety of oral semaglutide and hinted at a potential favorable CV mortality signal warranting further investigation.
SOUL: Semaglutide Outcomes Study [14]The SOUL trial, completed in 2024, expanded upon PIONEER 6 with a larger cohort of over 9,600 patients with T2DM and established CVD or multiple risk factors [14]. Participants were randomized to receive oral semaglutide or placebo and were followed for a median of 3.6 years [14]. This study demonstrated a statistically significant reduction in MACE (a composite of death from CV causes, nonfatal MI, or nonfatal stroke) compared to placebo among patients with T2DM and high CV risk. The incidence of MACE assessed in a time-to-first event analysis was 12.0% in the oral semaglutide group versus 13.8% in the placebo group (HR 0.86, 95% CI, 0.77–0.96; P = 0.006). There was a significant reduction in nonfatal MI (HR, 0.74; 95% CI, 0.61–0.90). However, there was no significant difference in nonfatal stroke (HR, 0.88; 95% CI, 0.70–1.11) or CV mortality (HR, 0.93; 95% CI, 0.80–1.09) between the groups. Additionally, oral semaglutide did not significantly reduce major kidney outcomes with event rates of 8.4% and 9.0% in the semaglutide and placebo groups, respectively (HR, 0.91; 95% CI, 0.81–1.05) [14]. These results suggest a favorable trend in CV outcomes consistent with studies of injectable semaglutides.
ACHIEVE-1: A Study of Orforglipron in Adult Participants With Type 2 Diabetes and Inadequate Glycemic Control With Diet and Exercise Alone [19]Orforglipron is a non-peptide, oral GLP-1 RA that binds to the GLP-1 receptor with high affinity and acts as a selective partial agonist [19]. The flexibility in dosing, lack of fasting requirements, and robust glycemic efficacy make orforglipron as a potential oral option. In ACHIEVE-1 trial, a phase 3, double-blind, placebo-controlled trial, once-daily oral orforglipron significantly reduced glycated hemoglobin (HbA1c) over 40 weeks in patients with T2DM managed with diet and exercise alone [19]. Mean HbA1c reductions ranged from − 1.24% to − 1.48% across the 3-mg, 12-mg, and 36-mg doses, compared with − 0.41% with placebo (P < 0.001 for all doses). Orforglipron was also associated with dose-dependent weight loss, with mean body-weight reductions of − 4.5%, − 5.8%, and − 7.6%, respectively, versus − 1.7% with placebo. There were no cardiovascular or renal outcomes evaluated in this study [19]. Ongoing phase 3 trials such as ATTAIN-Outcomes [22] is expected to address these endpoints.
Major Randomized Controlled Trials on Subcutaneous GLP-1 RAs for Cardiovascular and Renal Outcomes LEADER: Liraglutide Effect and Action in Diabetes:Evaluation of Cardiovascular Outcome Results [6]The LEADER trial enrolled 9,340 patients with T2DM and high CV risk. Once-daily subcutaneous liraglutide significantly reduced the incidence of the primary MACE outcome; CV death, nonfatal MI or nonfatal stroke, by 13% (HR 0.87; 95% CI 0.78–0.97), and CV death by 22% (HR 0.78; 95% CI 0.66–0.93) compared with placebo. Renal outcomes (defined as the new onset of persistent macroalbuminuria or doubling of the serum creatinine level accompanied by an estimated glomerular filtration rate (eGFR) ≤ 45 mL/min/1.73 m², the need for continuous renal-replacement therapy, or death from renal disease) also improved, with a 22% lower risk of new-onset nephropathy (HR 0.78; 95% CI 0.67–0.92), supporting both cardiovascular and renal protection [6].
SUSTAIN-6: Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes [7]SUSTAIN-6 randomized 3,297 T2DM patients to once-weekly subcutaneous semaglutide or placebo [7]. Semaglutide reduced the primary MACE endpoint (CV death, nonfatal MI, or nonfatal stroke) by 26% (HR 0.74; 95% CI 0.58–0.95), driven primarily by significant reduction in nonfatal stroke (HR 0.61) and nonfatal MI (HR 0.74). The trial also demonstrated renal benefits, with semaglutide reducing new or worsening nephropathy by 36% (HR 0.64; 95% CI 0.46–0.88), largely attributable to decreased progression to macroalbuminuria [7].
REWIND: Researching CardiovascularEvents With a Weekly Incretin in Diabetes [8]The REWIND trial included 9,901 participants, 69% of whom had no prior CVD, and followed them for a median of 5.4 years [8]. Once-weekly dulaglutide resulted in a 12% reduction in the primary MACE outcomes (CV death, nonfatal MI, or nonfatal stroke) (HR 0.88; 95% CI 0.79–0.99), demonstrating CV benefit even in a predominantly primary-prevention population. Renal outcomes (defined as the development of a urinary albumin-to-creatinine ratio > 33.9 mg/mmol in participants with a lower baseline value, a sustained ≥ 30% decline in eGFR [i.e., based on two consecutive eGFR measurements], or initiation of chronic renal replacement therapy) also improved, with a 15% reduction in composite kidney events (HR 0.85; 95% CI 0.77–0.93), mainly driven by reduced development of new macroalbuminuria [8].
EXSCEL: ExenatideStudy of Cardiovascular Event Lowering [23]EXSCEL evaluated once-weekly exenatide extended release in more than 14,000 T2DM patients [23]. The study met its non-inferiority requirement for cardiovascular safety but did not achieve superiority for reducing MACE (CV death, nonfatal MI, or nonfatal stroke) (HR 0.91; 95% CI 0.83–1.00). Although exenatide improved glycemic and weight outcomes, CV benefit was not statistically significant, and renal outcomes were not a primary focus [23].
ELIXA: Evaluation of Lixisenatide in Acute Coronary Syndrome [24]ELIXA enrolled 6,068 patients with T2DM shortly after an acute coronary syndrome. Using a 4-point MACE definition that included CV death, nonfatal MI, or nonfatal stroke and hospitalization for unstable angina, lixisenatide showed CV safety with no increased risk (HR 1.02; 95% CI 0.89–1.17), but without reduction of major CV events compared to placebo [24]. Renal outcomes showed modest reduction in albuminuria but no significant hard-renal endpoint benefits [24].
HARMONY Outcomes: Albiglutide andCV Outcomes in Patients with Type 2 diabetes and CV Disease [10]In 9,463 patients with established CV disease, once-weekly albiglutide reduced the risk of 3-point MACE (CV death, nonfatal MI, nonfatal stroke) by 22% (HR 0.78; 95% CI 0.68–0.90) [10]. Although albiglutide is no longer commercially available, HARMONY Outcomes provided evidence supporting GLP-1 RA-mediated cardiovascular protection in high-risk populations [10].
FLOW: A Research Study to See How Semaglutide WorksCompared With Placebo in People With T2DM and Chronic Kidney Disease [25]FLOW is the first dedicated renal outcomes trial for a GLP-1 RA, studying once-weekly semaglutide in patients with T2DM and chronic kidney disease (CKD). Semaglutide significantly reduced the primary composite kidney endpoint comprising renal failure, sustained decline in eGFR, or death from kidney/CV causes, by approximately 24% (HR 0.76; 95% CI ~ 0.66–0.88). In addition, semaglutide was associated with favorable effects on CV outcomes and all-cause mortality. These findings established semaglutide as the first GLP-1 receptor agonist to demonstrate kidney disease–modifying efficacy in a dedicated renal outcomes trial [25].
AMPLITUDE-O: Effect of Efpeglenatide on Cardiovascular Outcomes [9]AMPLITUDE-O enrolled 4,076 patients with T2DM and either established CV disease or CKD plus additional CV risk factors [9]. Using a 3-point MACE definition that included nonfatal MI, nonfatal stroke, or death from CV or undetermined causes, once-weekly subcutaneous efpeglenatide significantly reduced the risk of MACE compared with placebo (HR 0.73; 95% CI 0.58–0.92), meeting criteria for both non-inferiority and superiority [9]. Renal outcomes were prespecified secondary endpoints and included a composite of incident macroalbuminuria, an increase in urinary albumin-to-creatinine ratio of ≥ 30% from baseline, sustained decline in eGFR of ≥ 40% for ≥ 30 days, renal-replacement therapy for ≥ 90 days, or a sustained eGFR of < 15 ml per minute per 1.73 m2 for ≥ 30 days. Efpeglenatide significantly reduced the composite renal outcome compared with placebo (HR 0.68; 95% CI 0.57–0.79), with the benefit largely driven by lower rates of new-onset macroalbuminuria [9].
SURPASS-4: Efficacy and Safetyof Tirzepatide Once Weekly Versus Insulin Glargine in Patients With Type 2 Diabetes and Increased Cardiovascular Risk [26]SURPASS-4 enrolled 2,002 patients with T2DM and increased CV risk and compared once-weekly subcutaneous tirzepatide with insulin glargine [26]. CV safety was assessed using a 4-point MACE definition including CV death, nonfatal MI, nonfatal stroke, or hospitalization for unstable angina. Tirzepatide was not associated with an increased risk of MACE compared with glargine (HR 0.74; 95% CI 0.51–1.08), although the trial was not powered to assess CV superiority. Renal outcomes were not prespecified primary or secondary endpoints in this trial [26].
Guideline Perspectives and Clinical ImplementationThe American Diabetes Association and European Society of Cardiology (ESC) recommend injectable GLP-1 RAs with proven CV benefit for patients with T2DM and established CV disease or high CV risk [27, 28]. In 2019, the ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases assigned a Class I, Level A recommendation for the use of GLP-1 RAs in patients with T2DM and established atherosclerotic CV disease or at high or very high CV risk [29, 30]. Although more evidence is needed, oral semaglutide is now considered an alternative to injectable agents when administration barriers exist [28]. Orforglipron, pending CV outcome results, may expand the usage of GLP-1 RA therapy, particularly in primary prevention.
Comments (0)