
Remember me

Four positions were developed reflecting HCPs’ attitudes on counselling patients about hereditary cancer risk disclosure to relatives, visualised in Fig. 1. The positions illustrate different ways in which an HCP can approach counselling the patient and are distinct from one another based on variations in participants’ perspectives on risk disclosure, whether the responsibility lies ultimately with the patient or the HCP, and whether the HCP's focus during the consultation is on the current patient or ARRs.
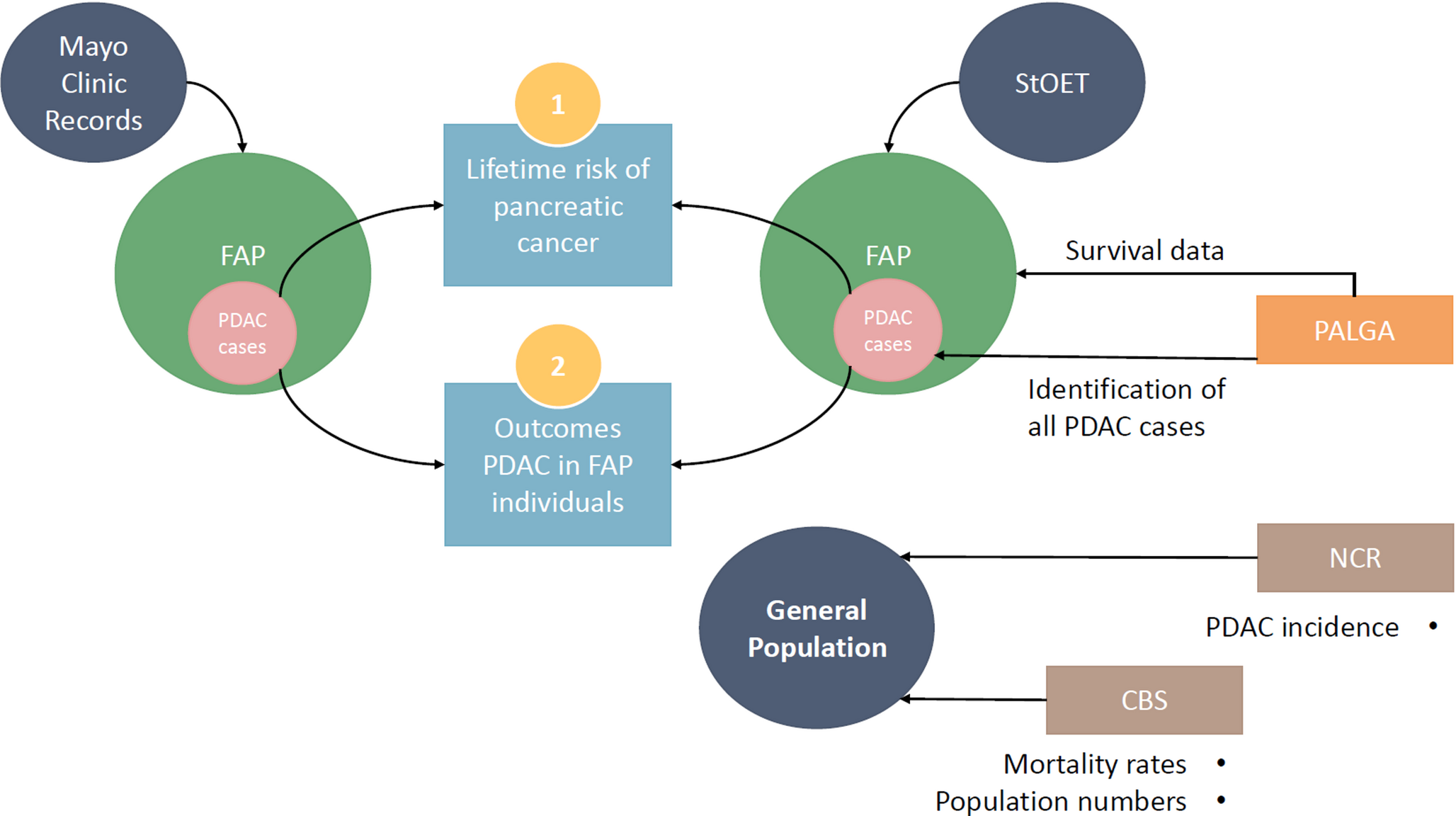
Fig. 1
Four positions describing HCP’s attitudes towards counselling patients about hereditary cancer risk disclosure to relatives. The standpoints are shown on a spectrum: the Y-axis is about who the HCP has in focus, and the X-axis is about how the HCP perceives the responsibility for relatives being informed. The positions are phrased as statements and shaped by the HCP’s profession, workplace and assignment but also by the perception of the patient’s health status and knowledge about relatives. HCPs described how they have, take, or move between these positions
A HCP’s position was partly dependent on their background and current workplace, as well as the clinical situation such as their perception of the patient's current health status, the family tree, and the characteristics of the cancer risk. This meant that a HCP could move between positions and hence counsel a patient regarding hereditary risk in various ways depending on the specific situation. The four positions should therefore not be understood as a fixed state of an individual HCP, profession or workplace but as fluid and situational. A general impression from the interviews was that the participants found their practice relatively well established and felt satisfied in managing their part of the patient’s genetic assessment. However, most of them had experienced recurrent situations, which they perceived as ethically complex.
Position 1: The patient is my one and only interest: ‘it´s clear and quite simple’In this position, the focus of the HCP was solely on the patient. The HCP provided basic pre-test information or post-test counselling to the patient but did not explain explicitly in dialogue the relevance for ARRs or explore the patient’s understanding of their responsibility but found it was sufficient to have provided information. In that sense, HCPs in this position had few doubts about their roles – the HCP was not responsible for ARRs, and it was up to the patient to decide if and how to share information. Counselling was hence perceived as ‘relatively easy’.
"I don't see it as my responsibility that potentially affected relatives undergo genetic testing, and it’s actually not my responsibility that they are informed about it either. It's actually the responsibility of the person in front of me; the responsibility lies with them. However, a lot of the responsibility for providing information [to the patient] does fall on me." (Participant no 11: Non-genetic HCP at a cancer genetics unit).
HCPs in this position took the patient’s perspective only, referring solely to the patient’s situation. HCPs in oncology care could refer to prioritising the patient’s medical situation, and that the consequences for ARRs were outside the scope of their assignment or expertise.
"We inform [the patient] that 'there was an error in a gene, but I can't really say if it affects you or not, but we will refer you to the cancer genetics unit’. That's what I say." (Participant no 8: Non-genetic HCP at an oncology care unit).
HCPs experienced in genetic counselling also adopted this position, being committed to the idea that the patient is solely responsible for ARRs. In-depth conversations about ARRs were not seen as their task, they viewed themselves as being neutral in relation to ARRs. HCPs could also acknowledge that there is an important relational aspect to family disclosure, emphasising that the patient probably needed to choose if and how to disclose risk in a considerate way. Another aspect was doubt about the extent to which healthy individuals benefit from predictive testing, which reinforced the idea that HCPs did not have a medical responsibility for disclosure.
I think ultimately, it's up to each person’s own judgment regarding what they want to know… I believe that as a healthcare unit, our role is to simply provide advice and support on how to obtain this information… But I can't quite say it's our ultimate responsibility to ensure it's disseminated. (Participant no 6: Non-genetic HCP at a cancer genetics unit).
Position 2: The patient and i are allies: ‘it´s a joint interest’In this position, which was commonly described, HCPs focused on their relationship as a caregiver to the patient but were also significantly engaged in the interest of ARRs.
” I am an oncologist, and … should only do that stuff. […]. And sometimes I have a patient where we found a genetic variant, and then all daughters had the same variant and had to go through the same process. Of course, it matters to the patient. I do think they are grateful that I ask about family members, how it went, and it matters to our relationship, also, I’d say.” (Participant no 5: Non-genetic HCP working at a cancer genetics unit and an oncology unit).
HCPs carefully considered how to best counsel the patient to be able to disclose risk to ARRs, including education about hereditary risk, assessment of the family tree and mutual exploring the relational aspects of ‘bringing bad news’.
“One can use general terms when speaking, like 'my experience tells me that in your situation, there are quite a few who feel this way or think this way.' This allows the patient to relate and perhaps open up to share their own thoughts and feelings. Sometimes, [the patient] can also feel shame, thinking, 'I should understand that it's not my fault [carrying a genetic variant], and I do, but still, I feel this way.' […] One can mention that we all carry different predispositions.” (Participant no 13, genetic HCP at a cancer genetics unit).
For HCPs in this position, patient autonomy and confidentiality were acknowledged, but at the same time they emphasised a professional stance that ARRs’ autonomy and agency should be guarded as well. They described building an alliance with the patient where disclosure to ARRs was a shared responsibility. If the patient was incapable of sharing information for any reason, HCPs tried easing the burden by postponing discussions about ARRs to a later consultation or by presenting alternative courses of action, such as discussing if another family member could help with disseminating information.
“It may be the case that the person themselves is dealing with a disease, undergoing treatment, and having a really tough time. They might not have much energy left, so I sometimes ask if they have a close relative, one who can help with spreading information, someone who is healthy and has a bit more resources at the moment. (Participant no 13, genetic HCP at a cancer genetics unit).
Position 3: The at-risk relative needs to know, but the patient is in charge:’it´s out of my hands’In this position, HCPs primarily considered ARRs need to be informed but understood disclosure as a task solely reserved for the patient. This often reflected a practical view of the responsibility of HCPs – if reaching ARRs had been an obligation, there would have been working models and resources. This 'hands-off' position could be described as static, with HCPs expressing feelings of resignation or an attitude of having the right to let go; a combination of duty of confidentiality, lack of formal duty, and the acknowledgement of the importance of the relational aspects of sharing hereditary information.
.…it depends on whether [the patient] is…, who this patient at the Clinical genetic unit […] is, how energetic or how caring he or she is. There is an inequality, or what to say, an unnecessary coincidence perhaps, that determines the outcome [for ARRs]. (Participant no 2, non-genetic HCP at both a cancer genetic unit and in oncology care).
Here, the patient was perceived as being in charge, and the HCP acknowledged the tension caused by the patient’s choice of whether and how to disclose for ARRs to access risk control.
"Imagine, if you sat there [diagnosed with breast cancer], as a sister or a cousin and… 'Darn, they didn't inform me… even though they did know I existed,' sort of. One has to think about this aspect and […] it has started to gain a bit more attention … it's a new era." (Participant no 5: Non-genetic HCP at a oncology care unit).
Further, non-genetic HCPs could consider initiating genetic testing in oncology care with the sole purpose of assessing heredity, but considering the patient’s wants or needs, where pushing for a DNA sample would not be the correct course of action. They could consider bringing up the issue of heredity with a relative accompanying the patient but not contacting other relatives who were not present.
Position 4: The patient is a means to reach the at-risk relative: ‘it needs to be done’In this position, HCPs focused on making sure the information was reaching ARRs. Their rationale was mainly the standpoint that carriers of genetic risk who could benefit from targeted risk programs should have the possibility to act upon it. HCPs’ expertise on risk was translated to a sense of duty, in some cases even a right, to warn ARRs. The patient could be seen as a means to reach ARRs. This duty was acknowledged by HCPs as not yet defined in guidelines, and direct contact was considered a future possibility.
“It is w who bear the greatest responsibility because we also understand how inheritance works […]. Even if someone claims to understand, they might have misunderstood something entirely. So, we can't rely on that. We know where the risks lie […]. Hence, we are aware of the risks and possess the expertise on what can be offered [risk management]. (Participant no 1, genetic HCP at a cancer genetics unit).
Moral nudging was described – telling the patient that disclosing information was the right thing to do or mentioning non-disclosure and its consequences if a relative was later diagnosed with cancer. A practical nudge could be handing over letters addressed to the family or contact info to be passed on to relatives. HCPs could suggest to the patient to identify relatives who could assist with risk disclosure, not to ease the burden, but rather to find ways to bypass the patient.
“[Many cancer patients] … struggle and endure and do what we tell them to do without saying that it's hard… So, I wish … that we were the ones who do it [disclosure to relatives]. That they can just let it go and feel that "now you [the HCP] take responsibility, you have found this and you know that they [relatives] benefit from it". I also think it’s natural that it should be our responsibility and not a private individual’s. (Participant no 2: non-genetic HCP with experience from cancer genetics assessments and oncology care).
Genetic HCPs commented on an ongoing discussion in the community about establishing direct contact with ARRs in selected situations. They also described the conflict between patient confidentiality and recurring situations of knowing about several ARRs – having to find a way to preserve confidentiality but also seeing to the interest of all parties being adequately assessed.
Comments (0)