FAP patients undergo a plethora of surgical and endoscopic procedures during their lifetime. Still, these patients are under perpetual risk of cancer formation, especially from duodenal and gastric adenomas. While some guidelines consider each ampullary adenoma as a candidate for endoscopic resection especially when exceeding 10 mm or with adverse histology [6], others recommend endoscopic resection only for a size ≥ 10 mm and with excessive growth [5]. These conflicting recommendations reflect the difficult balance between the avoidance of malignant progression versus periprocedural complications, mainly bleeding, perforation and acute pancreatitis. However, symptomatic ampullary adenomas with recurrent pancreatitis might justify even early endoscopic papillectomy [15], although recurrent pancreatitis might occur in FAP patients even without pancreatic obstruction by ampullary adenoma [16]. For an informed choice regarding papillectomy in FAP patients more data are needed about the success and complication rate and about risk factors for complications.
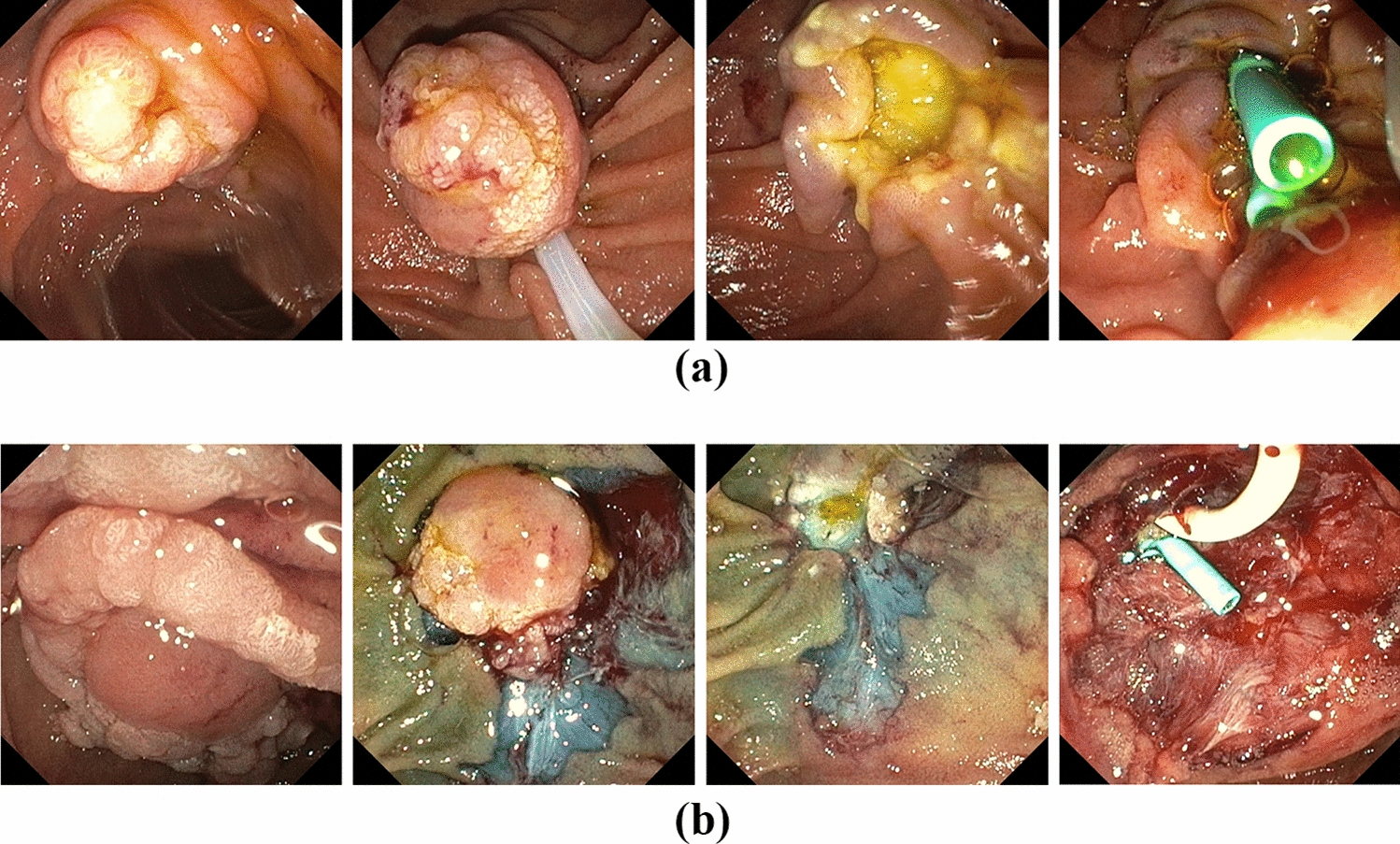
In our series, the percentage of laterally spreading adenomas was 45%, necessitating extensive additional resections by EMR and/or CSR for adenomas of up to 40 mm of size. Although a two-stage endoscopic resection has been recently published for large laterally spreading ampullary adenoma [10], we performed all combined resections in one single session. In these cases, we prefer to resect the lateral adenoma first, leaving the exposed papilla for final snare resection (Fig. 1b), although this might harbor a higher risk for perforation. However, our immediate perforation risk (2.5%) was comparable to pooled data from mixed cohorts (3.1%) [17] and FAP subgroups (2–3%) [3, 4], while a recent study reported a perforation rate of 21% [18].
Initial R0 resection rate of endoscopic papillectomy seem to be lower in FAP patients than in sporadic ampullary adenoma (64% versus 83%) [4] and as low as 36% when same-session adjunctive therapies were needed for complete resection [17]. Thus, high technical success rates of 95% in FAP patients in small case series might reflect a favorable patient selection [7], as larger series reported recurrence rates of only 48% in FAP patients [3]. Accordingly, in our series, 69% recurrence-free resection was achieved after a single session and 94% after repeated endoscopic resection and ablation techniques. This is in accordance with other studies reaching final recurrence-free resection after repeated interventions in 93% of FAP patients [4]. Many parameters have been discussed as risk factors for recurrence: genetic background (FAP), bile duct dilatation, periampullary resection, piece meal resection, adenoma size, and intraductal invasion [3, 7, 17]. Limited by our case number, none of these parameters were significantly associated with adenoma recurrence.
Intraprocedural bleeding was the most frequent immediate adverse event (33%) in our series and significantly associated with male sex. The association with insertion of a protective pancreatic endoprosthesis seems to represent a meta effect. Reported bleeding rates were much less and ranged between 11 and 13% [3, 4, 17]. In these studies bleeding was either defined by the established lexicon by the ASGE [19], which neglects transient bleeding episodes, or were not specified. Thus, our definition of bleeding with each event requiring an endoscopic hemostasis, has a lower threshold. In contrast, Le Bras et al. report a delayed bleeding episode after papillectomy in 26% of their patients [18] reflecting a twofold higher rate compared to our cohort.
Acute pancreatitis has been reported in 11–17% of papillectomies in FAP patients [3, 4] but cited with up to 20% in endoscopic guidelines [5]. We found an overall rate of pancreatitis of 25%, which was higher in patients with additional EMR/CSR (28%) than in single papillectomies (18%). However, in multivariate regression analysis, female sex and CSR were significantly associated with acute pancreatitis. This finding is in accordance with a 2015 published meta-analysis of 28 studies demonstrating an odds ratio of 1.46 for females regarding the post-ERCP pancreatitis rate [20, 21]. Whether female patients might benefit from a more aggressive fluid substitution as a prophylaxis for acute pancreatitis, needs to be investigated in prospective trials. BMI was not associated with the risk of acute pancreatitis. Although their protective effect is well established in larger cohorts [17], in our small series main pancreatic duct stenting was not associated with a lower risk of pancreatitis. However, prophylactic pancreatic stenting was technically successful in only 78%.
Long-term recurrence-free resection after a single procedure was high (74%) and nearly all relapsed adenoma could be endoscopically resected with a maximum of 2 additional interventions. Only 2 patients (6%) were not free of adenoma at the end of the surveillance. However, in one of these patients follow-up after therapeutic biopsy of a small adenoma relapse is still pending. Our recurrence rates are within the range of reported results of 21–48% [3, 4]. Despite repeated adenoma resection, recurrence forced surgery as a definite therapy in 2–13% of reported cohorts [3, 22]. In our cohort, none of the patients needed rescue surgery for adenoma recurrence so far. Known risk factors for adenoma recurrence are intraductal adenoma growth, bile duct dilation, and periampullary adenoma spread [3]. Due to the limited number of our cases, we could not confirm these risk factors on uni- or multivariate regression analysis.
Ampullary carcinoma are rarely found in the cohort of adenomas considered suitable for endoscopic resection (0–2%) but constituted 5% of our cohort. While one of these patients underwent curative rescue surgery, the other patient denied surgery and is still asymptomatic 746 days after endoscopic resection. Interestingly, while one carcinoma was detected within a 25 mm adenoma, the other one was found in a small ampullary lesion of 10 mm.
Endoscopic papillectomy shows high clinical success in FAP patients even with laterally spreading adenoma. Adenoma recurrence can be successfully treated with a limited number of reinterventions. Severe adverse events are rare and endoscopically manageable. In our cohort the most common additional resection technique was cold snare resection which might explain the higher immediate bleeding rate compared to other reports. However, the perforation and delayed bleeding rates reflecting complications with a more relevant clinical impact were much lower than recently published. Since female patients showed a higher risk for acute pancreatitis, these patients might benefit even more from prophylactic endoprosthesis application, non-steroidal antiphlogistics or forced intravenous hydration. As one carcinoma was detected in a 10 mm specimen with an intra-ductal extension of 5 mm, current thresholds for endoscopic papillectomy might be too strict for selected patients.


Comments (0)