Our study demonstrated that the stapled technique for RPC with IPAA required less operative time, resulted in fewer diverting ileostomies, and caused less anal incontinence compared to the hand-sewn technique. Despite the higher rate of adenoma recurrence in the stapled group, with frequent surveillance, recurrent adenomas could be effectively cleared endoscopically or surgically. Notably, progression to cancer at the ATZ occurred only in the hand-sewn group, leading to the inference that close surveillance is more critical for cancer prevention than the choice of anastomosis technique.
The choice between stapled and hand-sewn IPAA was primarily determined by the surgeon’s preference rather than patient-related oncologic factors. As summarized in Table 2, there were no significant differences between the two groups with respect to colon polyp density or the presence of cancer at the time of surgery, indicating that rectal polyp burden was not a major determinant of anastomosis type in this cohort. Some surgeons favored the stapled technique for its time- and function-saving advantages, while others selected the hand-sewn method to perform trans-anal mucosectomy, aiming to eradicate all potential adenoma recurrence risks [14]. To identify the optimal surgical technique, this single center retrospective study analyzed and compared the long-term oncological and surgical outcomes between the two anastomosis groups.
By tracking the long-term course of patients with adenoma recurrence, we found that remnant rectal mucosa in the stapled method was a significant risk factor for repeated adenoma recurrence. During endoscopic evaluations, the rectal stump left for anastomosis in the stapled group could be easily identified upon macroscopic examination [15]. Of the 14 cases of recurrent adenoma following initial removal, 13 cases were in the stapled group. Seven patients underwent more than four adenoma removal procedures, 6 of whom had undergone stapled IPAA. In three cases, multiple polyps (> 10) were detected, but complete removal was not done due to their benign looking appearance. Biopsies confirmed these polyps as tubular adenoma, low grade, and they were monitored with short-term follow-up endoscopy. We also reviewed the types of procedures used for adenoma clearance. In nine cases, trans-anal polypectomy under spinal or general anesthesia was performed when adenomas were too large for endoscopic removal and located close to the anus—all of these cases were in the stapled group.
Our study confirmed that a small amount of rectal mucosa, known as remnant rectal mucosa, could be left behind and cause adenoma recurrence, with the amount varying depending on the anastomosis technique [16]. In 2015, Ganschow reported that residual rectal mucosa was found more frequently after stapled IPAA compared to the hand-sewn method based on microscopic reviews of 100 biopsy cases [17]. Von Roon’s 2011 study also demonstrated that adenoma recurrence in the anorectal segment was more frequent and occurred earlier in the stapled group during a 10-year follow-up of 120 cases [8]. They also categorized adenomas larger than 10 mm and cancer cases, noting that one adenocarcinoma occurred, while nine high-risk adenomas were successfully treated with local excision. Other studies also have similarly demonstrated a higher risk of adenoma recurrence with stapled methods compared to hand-sewn methods [9].
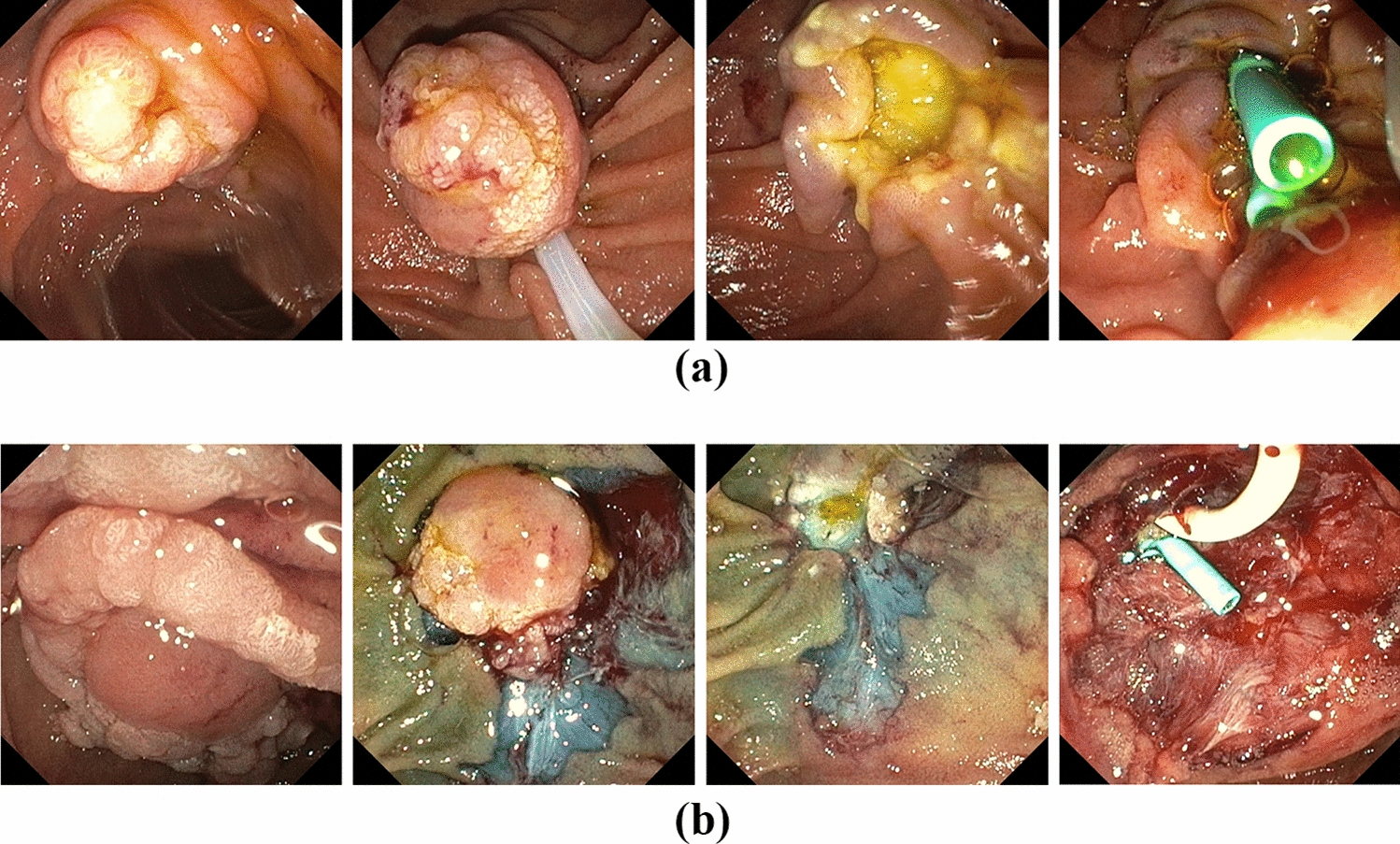
However, it is important to emphasize that, in our study, none of the patients with recurrent adenomas or multiple polyps developed adenocarcinoma in the stapled group. The median time to the first endoscopic surveillance was 20 months, indicating that patients typically received endoscopic follow-up within two years of surgery. More recent cases undergo endoscopy within six months, unless follow-up is lost or postoperative complications arise. This rigorous endoscopic surveillance appears to be preventing adenoma progression to cancer (Fig. 4). Previous studies have reported cases of cancer in residual rectal mucosa, but the proportion of adenomas progressing to cancer has remained very low [18,19,20].
In terms of surgical outcomes, stapled method was significantly faster (227.9 min vs. 324.5 min). The hand-sewn method prolongs surgery due to the mucosectomy and manual suturing required, and it is widely recognized that prolonged operative time can negatively affect patient prognosis [21,22,23]. Given the absence of a rectum in patients undergoing ileo-anal anastomosis, fecal incontinence is a major postoperative concern [24]. The Wexner score was used as a representative method of bowel function, and it was higher in the hand-sewn group, indicating worse anal function compared to the stapled group (3.43 vs. 1.54, p = 0.009).
To compare functional outcomes between the two groups, we also included complications related to bowel function such as ileus, recto-vesical fistula, and anastomosis disruption, while excluding non-bowel-related complications such as transfusion, pneumonia, and wound problem [25]. Although there was no significant difference in the overall complication rate between the two groups, major anastomotic complications occurred exclusively in the hand-sewn group. This aligns with many other studies suggesting that the stapled method offers better bowel function and time-saving advantages [26,27,28].
Several reports are consistent with our findings. In 2013, the Cleveland clinic compared the oncological and functional outcomes between two techniques, concluding that while the stapled method carried a higher risk of adenoma recurrence, it did not lead to a higher risk of carcinoma. In contrast, anastomosis stricture and fecal problem were more common in the hand-sewn method [10].
In our study, two patients from the hand-sewn group required pouch excision due to cancer development. One patient underwent abdominoperineal resection with pouch excision and lateral lymph node dissection after 20 months from RPC with IPAA due to lymph node metastasis detected on F-18 FDG PET-CT. This patient had sigmoid colon cancer at the time of initial RPC with IPAA. Metastatic adenocarcinoma from the sigmoid colon cancer was confirmed pathologically. This case is more appropriately considered a recurrence of the primary cancer rather than progression from adenoma. The other patient, diagnosed with sigmoid colon cancer 27 years ago, developed an adenoma at the dentate line 15 years postoperatively, which was removed endoscopically. After 10 years of follow-up loss, the patient presented with a large palpable anal mass, which was excised with ileal-pouch and confirmed as adenocarcinoma.
There are some limitations to our study. First, this was a retrospective study with a relatively small sample size. Our institution is a tertiary referral center, recognized as a large-volume cancer center in South Korea, performing approximately 1000 colorectal surgeries annually, including 500–600 operations for colorectal cancer. Considering that FAP accounts for approximately 1% of colorectal cancer cases, the number of cases in our cohort is not extremely small. On average, about four patients per year have undergone RPC with IPAA at our center; however, review of the most recent 3–5 years of surgical records shows that this number has increased to approximately seven cases annually. We anticipate that with continued systematic follow-up and case accumulation, a larger cohort will be available to further clarify the lifelong clinical course of FAP patients. Second, the Wexner score was obtained cross-sectionally, and because the time from the surgery varied between patients, it may not fully represent bowel function differences. A more systematic follow-up system is needed to collect functional outcomes of FAP patients over time. Third, we did not analyze the relationship between gene mutations and outcomes. For patients who underwent surgery more than 20 years ago, APC gene sequencing data were lacking. Future studies will explore the association between APC mutations and anorectal adenoma recurrence based on recent findings [29]. Fourth, the severity of polyp burden in the distal rectum might have influenced the choice of anastomosis technique. However, due to the retrospective design, detailed information on distal rectal polyp burden could not be retrieved, and it was therefore not possible to determine its impact on surgical decision-making. Nevertheless, as there was no significant difference in colon polyp density between the groups, we concluded that the choice of anastomosis type was more likely determined by surgeon preference rather than distal rectal polyp severity.
Our findings suggest that stapled IPAA, despite a higher risk of adenoma recurrence at the anal transitional zone, provides superior functional outcomes and shorter operative time compared to hand-sewn IPAA. Importantly, all recurrent adenomas in the stapled group were successfully managed without progression to carcinoma under regular endoscopic surveillance, underscoring the critical role of surveillance programs. A particular strength of our study is that both oncological and functional outcomes were assessed simultaneously, with oncological safety tracked over a lifelong follow-up period. Therefore, in centers where long-term endoscopic follow-up can be reliably implemented, stapled IPAA may be considered the preferred surgical option for FAP patients.


Comments (0)