
Remember me

We conducted in-depth, semi-structured interviews with 21 stakeholders between February 2024 and July 2024 (Table 1). The participants were 12 medical oncologists, three nurse practitioners, three clinical geneticists, two clinical laboratory geneticists and one health insurer. All healthcare providers were employed in the Netherlands by either an academic hospital, a teaching hospital or a general hospital and had varying amounts of experience in breast cancer care. Mainstreaming had been implemented in the hospitals of 13 of the 15 medical oncologists and nurse practitioners (87%). However, only three medical oncologists and one nurse practitioner stated that they were actually involved in discussing and ordering genetic testing. The other nine medical oncologists and nurse practitioners stated that surgical oncologists and nurse practitioners from the surgical department were responsible for discussing and ordering genetic testing. Genetic testing was discussed in a multidisciplinary team in the hospitals of 13 of the 20 participating HCPs (65%). However, only five of these 13 HCPs stated that a clinical geneticist was involved in the multidisciplinary team.
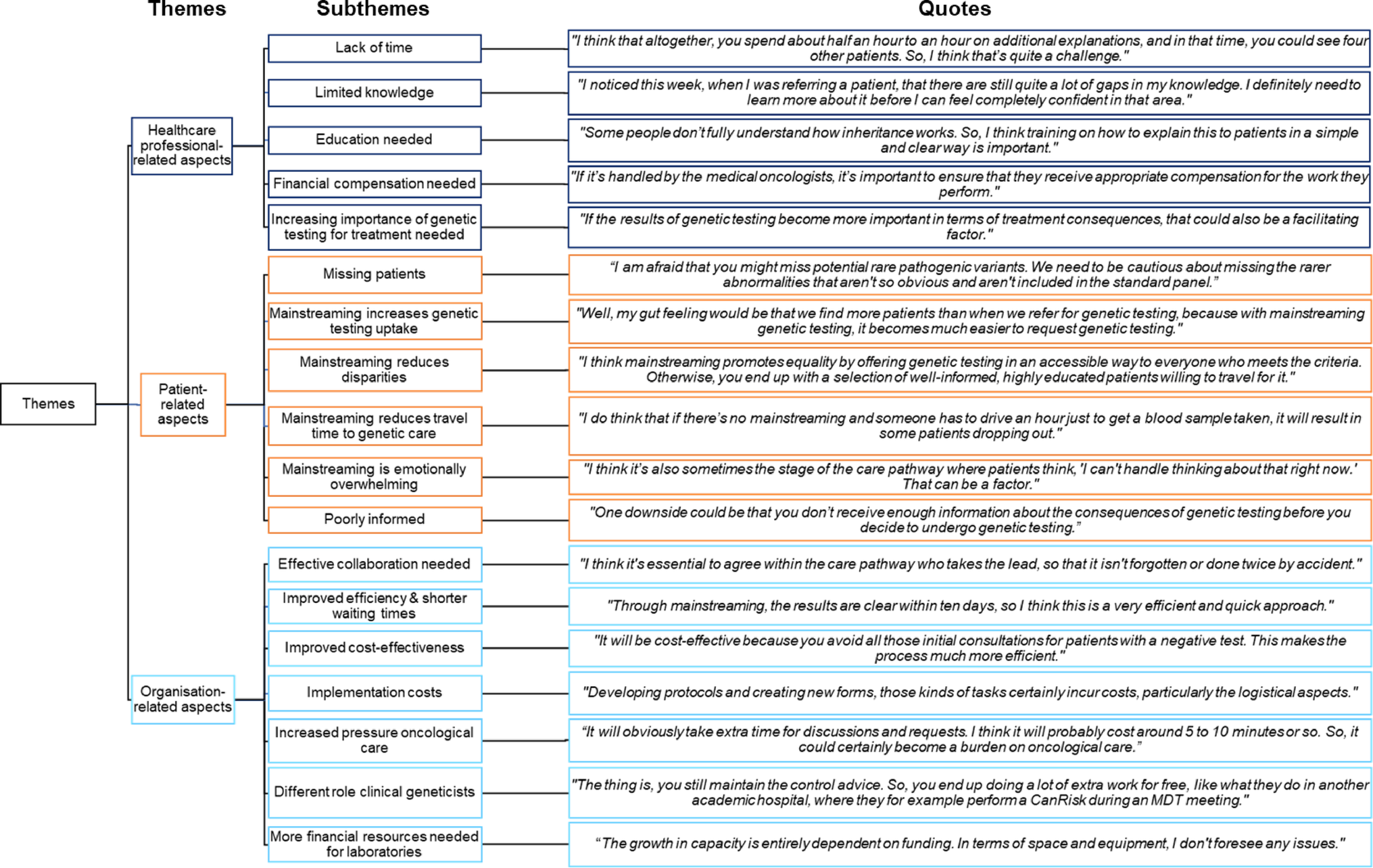
Table 1 Demographic overview of participantsThemesWe identified three overarching themes and 18 subthemes. In the following section, all subthemes are described according to the CTA framework, with a distinction between ‘healthcare professional-related aspects’, ‘patient-related aspects’ and ‘organisation-related aspects’. The themes identified from the interviews are presented in Fig. 1, each accompanied by a representative quote. These themes are also summarised in Table 2, along with the number of stakeholders who referenced each theme. Direct quotations are referenced by their corresponding numbers in Appendix 2 (e.g. Q1–5), providing the source for each statement.
Fig. 1
Overarching themes, subthemes and corresponding quotes
Table 2 Themes identified for further implementation of mainstreaming in breast cancer careHealthcare professional-related aspectsWe identified five subthemes related to the perspective of the HCP, comprising two barriers and three facilitators.
Lack of time (barrier)Lack of time was the most important barrier to further implementation of mainstreaming, mentioned by almost all medical oncologists and nurse practitioners. This could be due to either the additional administrative burden or, more importantly, an increase in consultation time (Appendix 2, Q1-5). A medical oncologist and a nurse practitioner already taking part in mainstreaming stated that the extra time investment was acceptable.
Limited knowledge (barrier)The majority of medical oncologists and nurse practitioners listed limited knowledge of breast cancer genetic counselling and genetic testing as a barrier. Limited ability in understanding the broad gene panels, explaining genetic testing, mapping a complete family history and answering patients’ specific genetics questions were also noted (Q6-9). One medical oncologist involved in mainstreaming noted that, while clinical geneticists possess more specialized expertise in the field, medical oncologists have sufficient knowledge to counsel patients effectively about genetic testing. Another medical oncologist involved in mainstreaming expressed a similar view, describing counselling about genetic testing as an integral component of breast cancer care.
Education needed (facilitator)The majority of participants stated that they felt confident in discussing genetic testing. However, education was highlighted as an important facilitator, noted by a third of medical oncologists and nurse practitioners. Most of them had a positive attitude to education about genetic testing. The key topic to be covered during education was the impact of genetic testing on the patient, including social, practical, financial and emotional consequences (Q10-13). Most of those willing to undergo education about genetic testing felt that a single educational session was sufficient, while others preferred ‘follow-up’ education or ‘learning on the job’ (Q14-15). Others found the availability of an eligibility criteria checklist and clear patient information to be helpful. Those hesitant about participating in the education were unsure of what could be gained from it.
Financial compensation needed (facilitator)Some medical oncologists said that financial compensation would be appropriate to account for the additional workload associated with mainstreaming (Q16-18).
Increasing importance of genetic testing for treatment needed (facilitator)Some medical oncologists also stated that the increasing importance of genetic testing for treatment selection could be seen to be encouraging HCPs to participate in mainstreaming, as in this case genetic testing would become more relevant for medical oncologists (Q19-20).
Patient-related aspectsFor the patient-related aspects, we identified six subthemes, comprising three benefits and three adverse effects.
Missing patients (adverse effect)The majority of participants stated that their perception was that only a limited number of eligible patients are not receiving genetic testing (Q21-23). Those who said otherwise noted that older patients (age > 50), patients with amendments to the family history or those who were unwilling to undergo genetic testing themselves are often the ones not receiving genetic testing (Q24-27). According to medical oncologists, eligible patients with metastatic breast cancer are frequently not offered genetic testing. Additionally, two medical oncologists stated that, in some cases, they chose to postpone discussing genetic testing with the patient (Q28-30). This could be because there was already too much to talk about during the first few consultations and it was then forgotten. Two clinical geneticists expressed concerns about potentially overlooking patients if genetic testing is requested by non-genetic HCPs. They worried that important clues in the patient’s family history or pathogenic variants in genes associated with rare cancer predisposition syndromes could be missed (Q31-32).
Mainstreaming increases genetic testing uptake (benefit)Most participants expected mainstreaming to increase the uptake of genetic testing (Q33-37). The most important reason for this was that mainstreaming makes genetic care more accessible, because patients do not need additional visits to another doctor (the clinical geneticist), who is sometimes even in another hospital (Q38-42). Another reason mentioned was that mainstreamed genetic testing would be forgotten less often. A few participants anticipated that the uptake would remain the same, as testing rates were already considered sufficient.
Mainstreaming is emotionally overwhelming (adverse effect)A possible drawback that was noted is that discussing genetic testing with the medical oncologist could be too emotionally overwhelming for patients (Q43-46), given that they are already receiving a large amount of information.
Poorly informed (adverse effect)Another disadvantage highlighted was that patients might be less well informed if genetic testing is discussed by a non-genetic HCP, leaving them with questions and a wish to consult a clinical geneticist (Q47-49).
Mainstreaming reduces disparities (benefit)More than half of the participants expected low socioeconomic status (SES) to have a negative impact on the uptake of genetic testing. Reasons given were that patients with high SES asked for genetic testing themselves more often and knew more about cancer prevalence (specifically breast cancer) in their families (Q50-53). A language barrier in the case of a migrant background or low literacy (including health literacy) was also listed (Q54). One medical oncologist mentioned a possible bias against discussing genetic testing with patients with low SES (Q55). Those who did not believe that SES was related to the likelihood of receiving a genetic test stated that they had no bias if the testing was clinically relevant and genetic testing was performed regardless of the patient’s SES. However, nearly three quarters of participants expected mainstreaming to have a positive effect on increasing accessibility of genetic care for patients with a low SES, making access to genetic testing more equitable (Q56-59).
Mainstreaming reduces travel time to genetic care (benefit)Opinions were divided about the effect that travel time to genetic care has on the likelihood of receiving a genetic test. Some stated that distance could be a barrier for certain patients, often due to limited options or restricted financial means. Others noted that the introduction of video consultations means that travel time is no longer a barrier (Q60-64). A third of the participants expected that introducing mainstreaming would have a positive effect on the accessibility and equitability of genetic care, due to a decrease in travel time and travel costs (Q65-66).
Organisation-related aspectsWe identified seven subthemes related to organisational factors that were one barrier, two facilitators, two benefits and two adverse effects.
Effective collaboration needed (facilitator)The most important facilitator mentioned by six medical oncologists and two clinical geneticists was setting up effective collaboration through well-defined agreements between different hospital departments and between genetic and non-genetic HCPs about the responsibilities for each part of the care pathway (Q67-70). Clear agreements about who is responsible for taking the patient’s family history and who is responsible for ordering genetic testing were mentioned.
Improved efficiency and shorter waiting times (benefit)Most participants expected mainstreaming to be faster and more efficient compared to referring a patient to a clinical geneticist (Q71-76). More than half of the participants expected that implementing mainstreaming would positively impact the capacity and waiting times for genetic care at the genetics department due to reduced referrals for consultations with clinical geneticists (e.g. only patients with a pathogenic variant or with a positive family history) (Q77-81).
Improved cost-effectiveness (benefit)Most participants anticipated that mainstreaming would be cost-effective, with the majority expecting a reduction in costs due to fewer clinical genetics consultations. Additionally, a reduction in the costs to society through breast cancer prevention in diagnosed patients’ families was also noted (Q82-85). Both of the clinical laboratory geneticists noted that there would be a relative decrease in costs, driven by greater efficiency resulting from higher testing rates. These differences, however, were expected to be limited (Q86). The health insurer representative added that the consultation rates for medical oncologists, surgical oncologists and nurse practitioners are lower than those for clinical geneticists (Q87).
Implementation costs (adverse effect)An adverse effect was noted in terms of the implementation costs of mainstreaming: educational, logistical and personnel expenses were identified as the most significant costs (Q88-89). Other challenges listed included an increase in the number of genetic testing requests for ineligible patients, resulting in higher costs (Q90-91). Some also suggested that mainstreaming could lead to higher genetic testing costs due to an increase in testing rates (Q92).
Increased pressure on oncological care (adverse effect)Another potential adverse effect that was mentioned was the increased pressure on oncological care, which was largely due to extended consultation times for oncologists, leading to delays in their schedules (Q93-96).
Different role for clinical geneticists (barrier)A barrier noted by one clinical geneticist was the concern that implementing mainstreaming could shift their role to a more consultative one. This shift could potentially result in the genetics department failing to meet the agreed number of consultations, which in turn might lead to decreased reimbursement through Diagnosis-Treatment Combinations (DBC), the Dutch variation of the Diagnosis-Related Group (DRG) system (Q97).
More financial resources needed for laboratories (facilitator)Both clinical laboratory geneticists noted that the increased number of genetic tests as a result of mainstreaming being implemented could strain the laboratory’s capacity, with financial resources being the primary concern. The increasing number of genetic tests performed for treatment purposes was mentioned as a factor. However, both clinical laboratory geneticists highlighted the potential for increased testing volume if financial resources could be increased. Additionally, both stated that it does not matter (from the laboratory’s perspective) who orders the genetic test (Q98-100).
Barriers and facilitatorsAmong the 18 subthemes, we identified three barriers and five facilitators to the implementation of mainstreaming for medical oncologists and nurse practitioners. We also identified five benefits and five adverse effects of mainstreaming (Fig. 2).
Fig. 2
The barriers, facilitators, benefits and adverse effects of mainstreaming based on participants’ perspectives
Comments (0)