This study investigated the effects of broadband elicitor duration on gain reduction using forward-masking psychoacoustic and TEOAE paradigms in adults with normal hearing. Direct comparisons were made between the measures of gain reduction, examining both their magnitude and time constants for individual subjects. We initially hypothesized that a positive correlation between physiological and psychoacoustic responses (i.e., magnitude effects), and between the physiological and psychoacoustic time constants of gain reduction would support the idea of a shared underlying mechanism—namely, gain reduction mediated by the MOCR. The methods of the current study were informed by previous psychoacoustic research employing tonal elicitors to characterize the temporal dynamics of gain reduction [41, 64]. These studies used on-frequency and off-frequency elicitors with durations ranging from 5 to 100 ms [41] or 10 to 150 ms [64], with a 4-kHz tonal signal. For most subjects, on-frequency elicitors produced maximal threshold shifts at durations of ~ 50 ms, beyond which the effects either plateaued or oscillated. In contrast, thresholds with off-frequency elicitors continued to increase with duration. Roverud and Strickland (2014) estimated time constants by applying a model that incorporated both a temporal integration window and a delay in the onset of gain reduction, yielding time constants ranging ~ 28 to 78 ms [64]. Given the maximal or near-maximal psychoacoustic gain reduction effect with ~ 50 ms on-frequency tonal elicitors, our previous studies adopted broadband elicitors of comparable duration. However, prior to the current study, the specific effects of broadband elicitor duration on psychoacoustic measures of gain reduction were largely underexplored. While this issue was introduced earlier, it is worth reiterating here: psychoacoustic studies have often employed broadband elicitors of longer durations (> 100 ms), or continuous elicitors, in an effort to maximize the MOCR response based on the time constants reported in OAE studies [23, 24]).
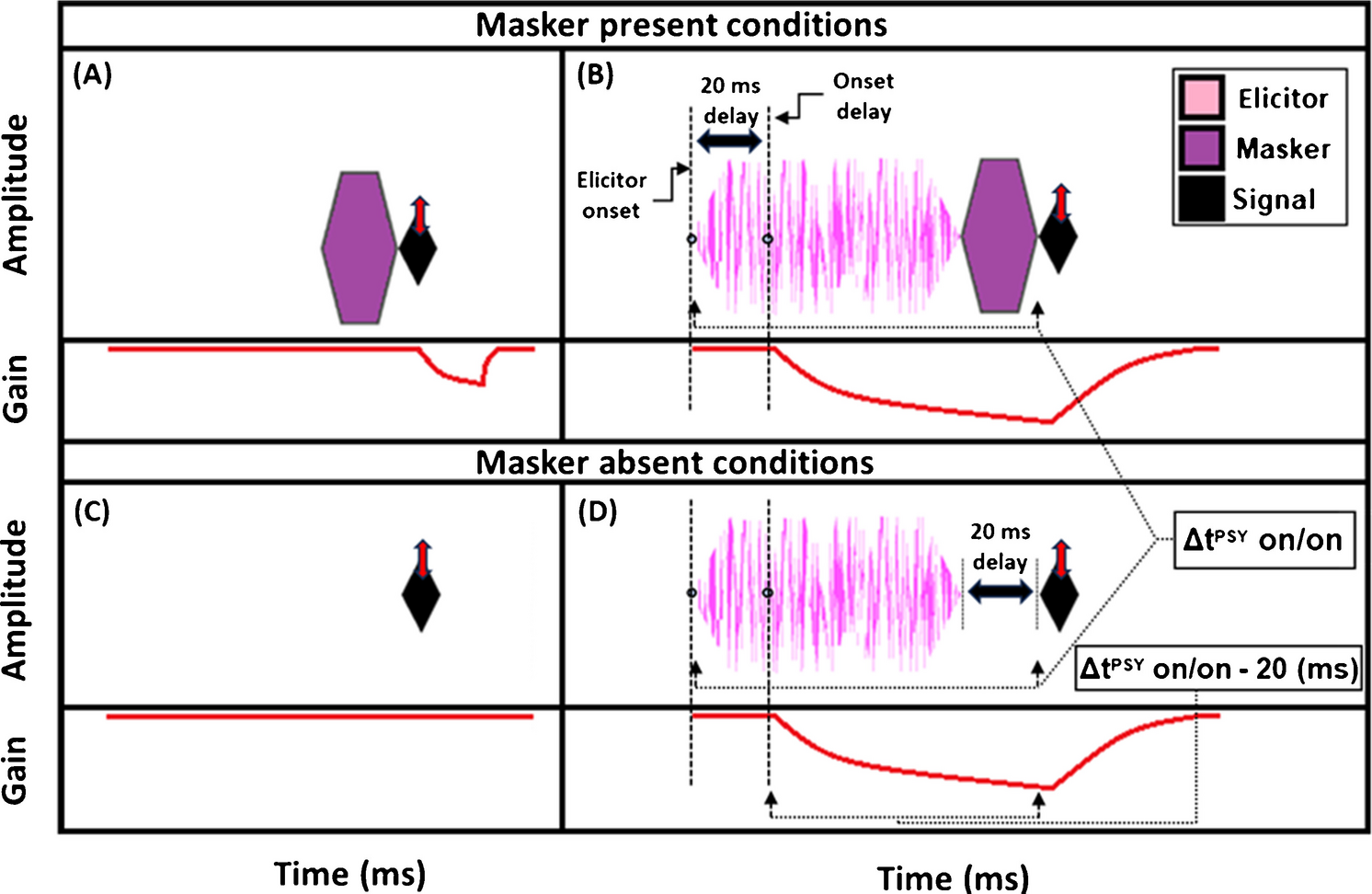
Psychoacoustic estimates of gain reduction ranged from ~ 4–7 dB for the masker present condition and ~ 5–9 dB for the masker absent condition, which increased with elicitor duration (Fig. 2). Physiologically, ΔTEOAEm+p was larger than ΔTEOAEm as a function of elicitor duration (Fig. 7), where ΔTEOAEm+p showed changes of ~ 1–1.5 dB, while ΔTEOAEm was typically less than 1 dB. The average psychoacoustic time constants were ~ 62–63 ± 7 ms (Fig. 4). Physiological time constants averaged ~ 53 ± 15 ms for the ΔTEOAEm+p condition and ~ 97 ± 24 ms for the ΔTEOAEm condition (Fig. 7). That is, when phase was accounted for in the TEOAEs, the physiological time constants closely matched the psychoacoustic time constants. However, when phase was omitted and only TEOAE magnitude changes were analyzed, the physiological time constants were nearly twice as long. Both psychoacoustic and physiological measures showed a buildup effect that increased with elicitor duration, reaching near-maximal levels within ~ 200 ms of elicitor onset. Exponential curve fitting effectively modeled both individual and group data, with most R2 values exceeding 90%.
While the psychoacoustic and physiological time constants were similarly short and consistent with cochlear gain reduction (possibly via the MOCR), our correlational analyses revealed that physiological responses were poor predictors of psychoacoustic responses across all elicitor durations. Most analyses showed non-significant, flat, or negatively trending relationships with elicitor duration when fitted by linear regression. This led to counterintuitive and mixed results when comparing elicitor-induced magnitude effects (ΔTEOAE and signal threshold shifts) and time constants of gain reduction. For instance, in terms of magnitude effects, ΔTEOAEm did not significantly predict signal threshold shifts in the masker present condition, as a function of elicitor duration (comparison 1; Fig. 8). In contrast, ΔTEOAEm+p significantly predicted signal threshold shifts in the masker absent condition, as a function of elicitor duration (comparison 2; Fig. 10). Interestingly, the relationships differed for the time constants of gain reduction: ΔTEOAEm was significantly positively related predictive of signal threshold shifts in the masker present condition (comparison 1; Fig. 9), whereas ΔTEOAEm+p showed a non-significant, flat relationship in the masker absent condition (comparison 2; Fig. 11). With multiple subjects not included in the correlational analysis due to poor fitting or considered as outliers, it unclear what this relationship would be with our original sample size (N = 19) or a larger subject pool as there is clear variation across subjects.
Comparing the Time Course of Gain Reduction to Other Psychoacoustic and Physiological Measures
The psychoacoustic and physiological time constants of gain reduction found in the current study (< 100 ms) align with the fast time constants of MOCR buildup previously measured using OAEs in humans (60–100 ms) [23, 24, 29, 30]. Similarly short time constants, in the tens of milliseconds, have been observed in animal studies with electrical activation of the OCB, including at the level of the basilar membrane [32] and the auditory nerve [33].
The psychoacoustic magnitude and time course data in the current study closely resemble those in our previous work. Salloom et al. (2023) used the same psychoacoustic paradigm and elicitor characteristics but employed a 4 kHz signal frequency, compared to the 2 kHz signal frequency in the current study. The time constants were ~ 46 ms for the masker-present condition and ~ 78 ms for the masker-absent condition. In both cases, the buildup of threshold shifts was maximal or near-maximal within approximately 200 ms of elicitor activation [34].
One prior psychoacoustic study examined forward masking of a 6-kHz tonal signal using broadband noise maskers of varying durations (5, 10, 30, and 200 ms) [58]. One configuration included a 20 ms delay between masker offset and signal onset, identical to the no masker condition used in current study. Maskers were presented either 0 dB spectrum level (approximately 40 dB SPL) or 40 dB spectrum level (approximately 80 dB SPL). At 0 dB spectrum masker level, two of the four subjects exhibited maximal masking for the 30-ms masker, followed by reduced masking with the 200-ms masker-showing an oscillation pattern. The other two subjects showed no consistent change in masking effectiveness across masker durations (i.e., flat). At 40 dB spectrum masker level, two subjects exhibited increased masking with increasing masker duration, while the other two subjects showed plateauing responses for the 30 ms masker. Of the latter two subjects, one subject showed reduced masking at 200 ms, while the other showed a continued plateau. Taken together, these observed patterns—increased masking with masker duration, oscillatory masking effects, and early plateaus—are qualitatively consistent with trends seen in our psychoacoustic experiments. However, the masker durations tested in that study did not include intermediate durations between 30 and 200 ms, nor durations longer than 200 ms. As a result, it is difficult to determine whether the observed plateaus reflected the peak of the masking function or whether masking would have continued to change with longer masker durations.
The temporal properties of gain reduction observed in the current study align with findings from Walsh et al. (2010), who measured the “overshoot” effect using a psychoacoustic paradigm and a modified SFOAE paradigm (the nSFOAE) [37]. Overshoot refers to the phenomenon where a tonal signal presented at the onset of a masker is less detectable than when preceded by an additional sound, known as an elicitor [77]. In the Walsh et al. study, both paradigms used a 4-kHz tonal signal and a 400-ms broadband noise masker. The psychoacoustic measurements and SFOAE responses exhibited similar time constants of approximately 65 ms and 72 ms, respectively. Additionally, individual data revealed maximal or near-maximal buildup of the overshoot effect when the signal was delayed by ~ 100 ms from masker onset [37]. These temporal overshoot effects are similar to the time course of our psychoacoustic and TEOAE measurements, suggesting similar mechanisms (gain reduction possibly via MOCR). For clarification, in the Walsh et al. study, as the temporal gap between the elicitor and the probe signal increased, both the nSFOAE SNR and behavioral detection sensitivity improved, indicating that the MOCR was likely contributing to a greater reduction in cochlear sensitivity to the masker than to the signal. While overshoot is measured in simultaneous masking paradigms where MOCR activation may enhance detectability, the current study used forward masking, which involves an increase (worsening) in behavioral thresholds and a reduction in TEOAE amplitude.
Gain reduction effects with broadband elicitors often required longer durations (~ 150–200 ms) to reach maximal or near-maximal levels, with small but continued growth in most subjects (see Fig. 3). A previous study has shown a shorter time course for an on-frequency elicitor than for an off-frequency elicitor nearly an octave below the signal frequency [41]. Previous research has shown that broadband elicitors reduce cochlear gain [51] and broadens cochlear tuning [44]. As gain reduction broadens cochlear filters, the decrease in gain at the tip of the filter may be offset by the widening of the filter, making the effects of broadband elicitors similar to the off-frequency elicitor conditions used by Roverud and Strickland, 2010 [41]. The interplay between these factors likely explains the oscillation in signal threshold shifts and ΔTEOAE with elicitor duration observed in some subjects. These findings suggest that the time course of gain reduction depends on the specific characteristics of the elicitor used to evoke the effect including its frequency relative to the signal and its overall bandwidth [78]. The current study was limited to elicitor durations of 800 ms in the psychoacoustic experiment and 400 ms in the TEOAE experiment, and it is unclear if longer duration elicitors would have had any significant effect on the responses.
Considerations for the Lack of Correlation Between Physiological and Psychoacoustic Gain Reduction
Consistent with the correlational results of the current study, previous research examining the relationship between psychoacoustic and otoacoustic measures of MOCR gain reduction has yielded mixed and often inconclusive results. Below, we describe studies that used metrics comparable to those in the current study, focusing on elicitor-induced magnitude changes on the response. We also discuss possible reasons for the inconsistent results across these studies and the current one. Studies comparing speech perception in noise tasks to changes in OAE levels are beyond the scope of this research and are not discussed here. Psychoacoustic tasks used in these comparisons are thought to reflect gain reduction or related mechanisms when an elicitor is present, including overshoot [37, 50], signal intensity discrimination [49], signal threshold in quiet [46], and PTCs [43, 44]. Most studies found no significant relationship between psychoacoustic and physiological measures [44,45,46, 50]. However, some reported significant positive relationships between the two measures [37, 43, 49].
Several factors may explain the mixed results regarding the relationship between psychoacoustic and physiological measures of gain reduction. One key issue is the considerable variability in methodologies and stimuli across studies. For example, some studies used simultaneous masking paradigms [37, 44, 50], which inherently involve two-tone suppression. This makes it difficult to disentangle the contributions of MOCR activation from those of two-tone suppression. Even when methodologies and stimuli were similar between studies, their overall results conflicted from one another (e.g., [37, 50]). Furthermore, the type of otoacoustic emission (OAE) paradigms also varied widely in these studies. Some studies measured changes in distortion-product OAEs (DPOAEs; [2f1-f2 amplitude]; [43, 44], while others focused on transient-evoked OAEs (TEOAEs; [45, 49]), stimulus-frequency OAEs (SFOAEs; [37, 50]), or a combination of TEOAEs and DPOAEs [46]. Importantly, DPOAEs do not share the same primary generation mechanism as TEOAEs and SFOAEs [71], raising questions about how these differences impact the results in those studies. Additionally, it is unclear how much of a factor OAE probe calibration methodology varied across these studies, as it can be a significant factor in the reliability of measurements [66, 67].
Most studies employed contralateral elicitors to activate the MOCR [43,44,45,46, 49], which avoids excitatory masking effects on the probe in the ipsilateral ear. In contrast, overshoot studies used ipsilateral stimuli [37, 50]. Ipsilateral elicitors produce significantly larger gain reduction effects psychoacoustically [51] and have different effects on otoacoustic responses than contralateral elicitors [25, 70]. For example, the OAE phase changes by the MOCR has been shown to differ depending on the laterality of the elicitor [25, 70], and the change of OAE amplitude by the MOCR may differ depending on elicitor laterality and the elicitor bandwidth [28]. It remains unclear whether elicitor laterality influenced the results of these studies. Other potential factors include inherent variability in participants' responses and small sample sizes, with many studies including 12 or fewer subjects. High-variance data combined with low sample sizes reduces statistical power and can affect the reliability of inferential conclusions. Variability in MOCR data may stem from differences in neural responses [26, 40, 55, 56, 79, 80], or from the methodology and analyses used to measure MOCR effects [46, 56, 68].
With many of these potential factors we outlined here, in our view, Marrufo-Pérez et al. (2021) conducted the most well controlled and robust study comparing a psychoacoustic task thought to be related to MOCR gain reduction (signal in noise task) and measuring the change in TEOAE and DPOAE IO function by the elicitor. The tone detection task was signal threshold in quiet with and without a 60 dB SPL long duration broadband contralateral elicitor (850 ms duration; 0.01–10 kHz bandwidth). Pure tone frequencies were 0.500, 1.5, and 4 kHz (each 300 ms in duration). The signal started 500 ms after the elicitor onset when the elicitor was present, allowing for MOCR build to fully activate. For all signal frequencies, the addition of the elicitor increased signal threshold. TEOAE and DPOAE IO functions over a range of click levels (48–60 dB pSPL) and over a range of levels of primary tone f2 (30–50 dB SPL) with the level of primary tone f1 at a level ratio relative to f2 (L1 = 0.4*L2 + 39 dB SPL), respectively. They measured these functions with and without the presence of the elicitor, where the elicitor was longer than in the behavioral experiment, and was continuously presented contralaterally during the elicitor present condition for both TEOAEs and DPOAEs. TEOAE level was estimated in various frequency bands, including 1, 1.5, 2, 3, 4 kHz. Primary f2 frequencies were 1, 1.5, 2, 3, and 4 kHz, with a f2/f1 ratio fixed at 1.2. They found that the elicitor suppressed the OAE at all frequency bands (TEOAEs) and f2 frequencies (DPOAEs) tested, respectively [46].
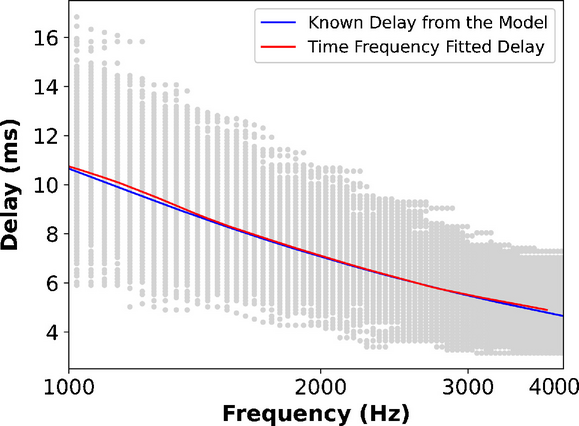
Most OAE studies measuring MOCR effects estimate the suppression of the response, which is the decibel change or percent change of the OAE magnitude by the elicitor, and is known as the vertical displacement of the OAE on the cochlear IO function (see Supplementary File 1; Supplementary Fig. 1D; [46] their Fig. 1). Marrufo-Pérez and colleagues note that comparing the elicitor induced signal threshold increase in behavior to the negative decibel change would not be a fair comparison, because their behavioral task measures the horizontal shift (“effective attenuation”) while suppression of OAEs would measure the vertical shift of the cochlear IO function. Therefore, they quantified the horizontal displacement of the TEOAE and DPOAE IO functions by fitting straight lines to their functions, with and without the elicitor. It should be noted that differences in horizontal and vertical displacement likely occur over the compressive part of the IO function (for mid- and high probe and signal levels), but the horizontal and vertical displacement should be the same when the probe and signal levels are on the lower linear part of the IO function [46, 68].
Horizontal displacement of the TEOAE IO function was calculated by estimating the TEOAE level in the fitted line without the elicitor produced by a 54 dB pSPL click followed by the click level on the TEOAE IO function with the elicitor present that produced the same TEOAE level (often estimated by extrapolation). TEOAE IO horizontal displacement is the difference in click level between these two conditions [46, 68]. DPOAE IO horizontal displacement was calculated similarly, where the displacement was estimated relative to the DPOAE response for the L2 = 35 dB SPL. Both of their TEOAE and DPOAE probe levels are on the lower portion of the IO function. Correlational comparisons were made between the TEOAE and DPOAE IO curve horizontal displacements and the tone threshold shifts by the elicitor. These comparisons were made at 1.5 kHz and 4 kHz, corresponding to the TEOAE frequency band, the DPOAE for the f2 frequency, or the psychoacoustic signal frequency. Overall, none of their comparisons were statistically significant, and the relationship between the measures in all comparisons trended towards being flat. Their findings are in despite of each of their measures producing effects that are consistent with MOCR activation by a contralateral broadband elicitor (an increase in signal threshold and decrease in OAE magnitude), they used comparable methodology between their psychoacoustic and physiological measures, they compared the horizontal displacement for fair comparison, and they compared relatively large sample sizes (7–9 subjects at 1.5 kHz, and 13–15 subjects at 4 kHz). The results from Marrufo-Pérez et al., 2021 are nearly identical to the results of the comparisons made in the current study. This suggests that even highly controlled and robust studies, such as the Marrufo-Pérez et al., 2021 study and the current study, psychoacoustic and otoacoustic estimates of the magnitude of MOCR gain reduction are unlikely to positively correlate even though both measures activate the MOCR.
We note that individual IO functions, measured psychoacoustically and by OAEs, can vary across subjects. The linear and compressive regions, as well as the knee point separating them, are not fixed in level and may differ from one individual to another. Because we used a single probe click level, we were unable to determine whether the measurements in each subject were part of the linear or compressive portion of the IO function. It is possible this may have added to the variability found in the subject responses. Nonetheless, based on our preliminary testing of TEOAE magnitude and click-level effects, and findings from similar TEOAE paradigms, the choice of a 54 dB FPL probe level provided a reasonable trade-off between TEOAE signal-to-noise ratio and the magnitude of observable MOCR effects (Supplementary File 1; Supplementary Fig.

Comments (0)