Correction of oblique astigmatism poses a distinct clinical challenge due to the need for precise correction of both magnitude and axis [10,11,12,13,14]. Unlike the relatively straightforward correction of spherical myopia, oblique astigmatism is highly sensitive to axis misalignment, cyclotorsional movements, and biomechanical variations [11]. In this study, both Small Incision Lenticule Extraction (SMILE) and toric Implantable Collamer Lens (ICL) implantation demonstrated favorable safety and efficacy profiles for the correction of myopic oblique astigmatism. However, our findings suggest that toric ICL implantation may offer more predictable outcomes, even at moderate levels of preoperative astigmatism.
Efficacy
At six weeks postoperatively, both groups showed excellent efficacy. The mean efficacy index was 0.97 ± 0.17 in the ICL group and 0.94 ± 0.15 in the SMILE group (p = 0.18). A postoperative uncorrected distance visual acuity (UDVA) equal to or better than preoperative corrected distance visual acuity (CDVA) was achieved in 83% of eyes in the ICL group and 79% in the SMILE group.
These findings underline the high efficacy of both methods for patients with oblique astigmatism.
Our findings are supported by a recent comparative analysis of FDA-reported outcomes, which evaluated SMILE, Toric ICL, and topography-guided LASIK (TG-LASIK) in the treatment of myopia and myopic astigmatism. In that study, all three modalities demonstrated high efficacy, with SMILE achieving significantly better accuracy for cylinder correction compared to Toric ICL across multiple thresholds (within ± 0.25 D, ± 0.50 D, and ± 1.00 D; all p < 0.01) [15]. These findings align with our results. Together, these data reinforce the suitability of both SMILE and ICL for effective visual rehabilitation in myopia, including eyes with oblique astigmatism.
These findings are in line with prior comparative studies of T-ICL, femto-LASIK, and SMILE in patients with myopic astigmatism. In a prospective study by Ganesh, all three modalities achieved effective astigmatism correction at one year, with mean residual cylinder values of –0.21 ± 0.28 D (T-ICL), − 0.17 ± 0.36 D (FS-LASIK), and − 0.22 ± 0.28 D (SMILE), showing no statistically significant differences in predictability (p > 0.05). In that study, 97% of SMILE-treated eyes and 93% of T-ICL eyes achieved UDVA of 20/20 or better, which aligns closely with our efficacy outcomes. Interestingly, the greatest gain in CDVA was observed in the T-ICL group, despite a small number of eyes requiring lens exchange due to rotation and vault-related issues. These results support the overall high efficacy of both SMILE and ICL, while also highlighting the importance of meticulous preoperative planning in phakic IOL implantation to minimize the risk of postoperative adjustments [16].
Safety
The safety index was similarly high, with 1.02 ± 0.11 for ICL and 1.01 ± 0.09 for SMILE, and no eye in either group lost more than one line of CDVA. These findings align with numerous studies that have consistently reported excellent safety outcomes for both SMILE and toric ICL procedures [16,17,18,19,20,21].
Accuracy
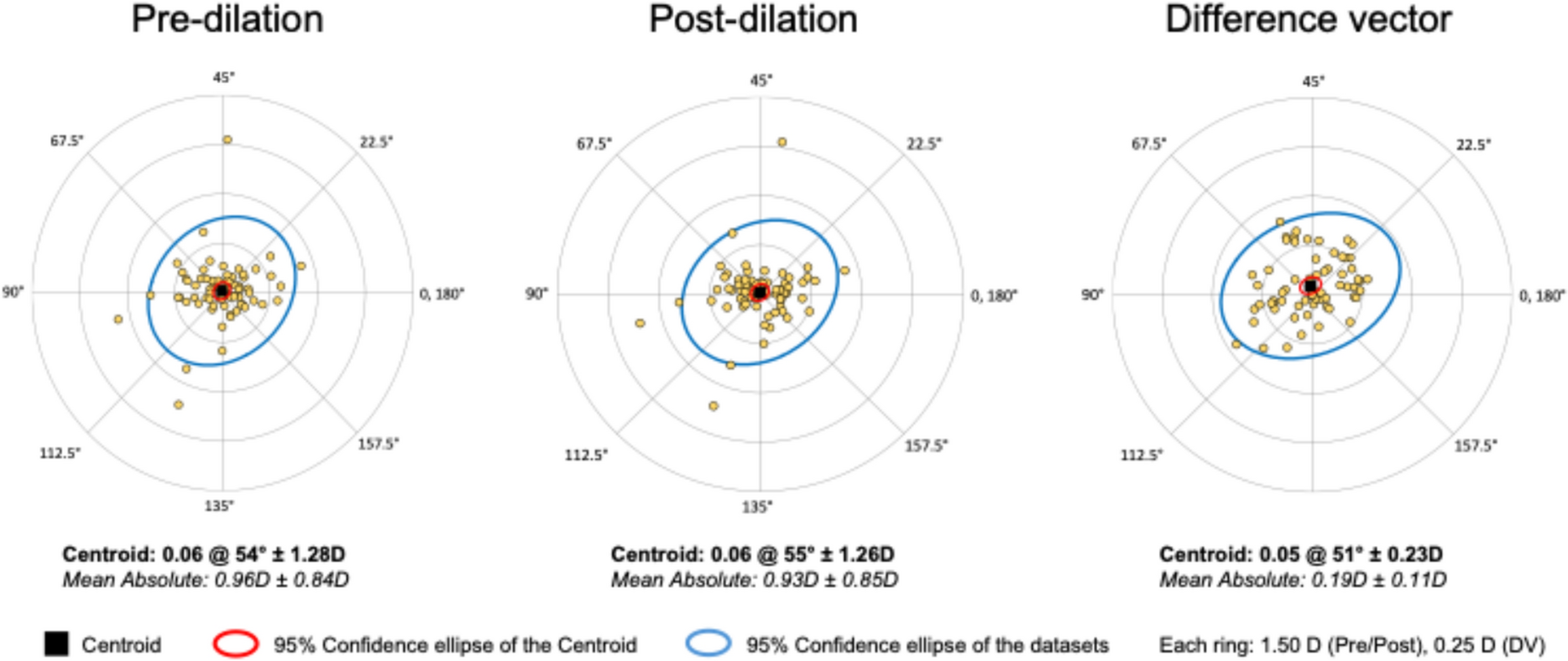
Regarding refractive accuracy, 85.7% of ICL eyes and 81.4% of SMILE eyes were within ± 0.50 D of the intended spherical equivalent. The mean achieved SEQ was 0.07 ± 0.44 D in the ICL group and − 0.16 ± 0.41 D in the SMILE group. Vector analysis revealed a mean correction index (CI) of 0.97 ± 0.32 in the ICL group and 1.04 ± 0.34 in the SMILE group (P = 0.48). The regression slope of surgically induced astigmatism (SIA) versus target-induced astigmatism (TIA) was 1.04 in the ICL group (R2 = 0.77) compared to 0.76 in the SMILE group (R2 = 0.67), indicating stronger vector predictability with ICL. Additionally, At one year postoperatively, both SMILE and toric ICL demonstrated excellent refractive stability, with no clinically significant regression or loss of visual acuity. The minor additional reduction in cylinder observed in the ICL group (mean ≈ 0.1 D, p = 0.044) likely reflects subtle long-term axis stabilization rather than true regression.
the angle of error (AE) was lower in the ICL group, with 76% of eyes falling within ± 15° of the intended axis, compared to 82% in the SMILE group (P = 0.43). These results align with the findings of Ganesh et al., who reported comparable refractive predictability among T-ICL, femto-LASIK, and SMILE at one year [14, 16].
Our findings are further supported by a recent refraction-matched comparative study evaluating SMILE and ICL implantation for high myopia, which reported superior refractive predictability and visual quality in the ICL group. In that study, 90% of ICL-treated eyes achieved a spherical equivalent within ± 0.50 D of target, compared to 72.5% in the SMILE group (p = 0.045), confirming the higher precision of ICL in matching the intended refractive outcome. This aligns well with our own data. Additionally, the ICL group in that study showed significantly higher efficacy and safety indices, along with lower induction of higher order aberrations. Notably, patients in the ICL group reported fewer subjective visual disturbances such as starbursts and fluctuations of vision, supporting the qualitative advantage of ICL in visual performance. These findings emphasize that, while both procedures are highly effective, ICL may offer more consistent refractive accuracy and improved patient-reported visual quality, particularly in cases requiring high precision [20].
To confirm the adequacy of the sample size, a post hoc power analysis for CI was conducted. Based on the observed effect size (Cohen’s d = 0.48) and sample size of 70 eyes per group, the achieved power was 80.5%, indicating that the study was adequately powered to detect clinically relevant differences in astigmatic correction.
Postoperatively, SMILE produced outcomes in UDVA and SEQ comparable to FS-LASIK and transepithelial PRK (t-PRK), while demonstrating lower surgically induced astigmatism and coma index in other studies [22]. These advantages are attributed to its flapless approach and minimal epithelial remodeling, preserving corneal biomechanics and asphericity. However, despite these optical benefits, our data revealed higher residual cylinder and less predictable astigmatic correction with SMILE compared to ICL, likely due to the absence of real-time cyclotorsional alignment and reliance on manual centration.
A key limitation of the SMILE procedure is its lack of automated cyclotorsion compensation and intraoperative axis control. These limitations can result in axis misalignment during treatment, particularly in cases of oblique astigmatism, where small deviations can lead to significant undercorrection [23]. Recently, cyclotorsion tracking has been implemented in the ZEISS VISUMAX 800® platform. This system integrates OcuLign technology, which enables automatic compensation for cyclotorsion by detecting and correcting rotational misalignment intraoperatively. The addition of this feature represents a significant technological advancement, particularly for improving the accuracy of astigmatic correction in SMILE procedures. In patients with higher cylinder values, both procedures exhibited a tendency toward undercorrection, which was more pronounced in the SMILE group. This observation aligns with findings by Chow et al. and Ivarsen et al., who reported undercorrection rates of 13–16% per diopter in high astigmatism cases after SMILE.
In contrast, toric ICL implantation provides astigmatic correction independent of corneal shape and biomechanics. This may explain the more reliable axis alignment and lower residual cylinder observed in our ICL group. These findings are in line with previous studies by Shimizu et al. and Kamiya et al., who reported higher predictability and rotational stability with toric ICLs, especially in cases of high myopic astigmatism [24, 25]. One potential limitation of toric ICL treatment is the risk of postoperative lens rotation, which can lead to residual astigmatism and reduced visual quality [26]. Studies have shown that every 3° of rotational misalignment reduces the effectiveness of astigmatic correction by approximately 10%, with rotations greater than 10° significantly compromising visual outcomes [27, 28].
Undercorrection of astigmatism following SMILE surgery has been well-documented in the literature. Multiple factors may contribute to reduced astigmatic correction efficacy, including cyclotorsional misalignment, centration errors, and the magnitude of preoperative astigmatism. Researchers have proposed various strategies to address this issue [11, 13, 29,30,31]. No standardized nomogram protocol is widely accepted, leading to variability in refractive outcomes, particularly in cases of oblique or high astigmatism. Oblique astigmatism remains especially challenging, with no routinely adopted nomogram adjustments to date. In this context, our findings provide clinically meaningful data to support refinement of nomogram strategies for oblique astigmatism, where precise alignment and magnitude correction are crucial to achieving optimal outcomes. Recently Yu et al. developed and validated a regression-based nomogram for the correction of high myopic astigmatism using SMILE surgery. Their method was based on a linear regression between target-induced astigmatism (TIA) and flattening effect (FE), applied to 112 eyes with astigmatism ranging from − 2.75 to − 4.50 D. Compared to a control group of 143 eyes treated using manifest refraction alone, the nomogram group showed significantly higher accuracy, with 97% of eyes within ± 0.50 D of residual astigmatism versus 89% in the control group (P = 0.010). The angle of error was also improved, with 100% of eyes in the nomogram group within ± 5°, compared to 95.8% in the control group (P = 0.028). Vector analysis demonstrated reduced undercorrection in the nomogram group (mean 2.7% overcorrection) compared to the manifest group (mean 8.4% undercorrection). These findings support the clinical utility of regression-based nomogram refinement for enhancing predictability in high astigmatism SMILE treatments [32].
To mitigate cyclotorsional effects in SMILE, methods like limbal marking and head positioning have been suggested, but these are manual and lack consistency. In contrast, toric ICLs allow for precise preoperative planning and offer greater rotational stability, reducing susceptibility to misalignment.
Our findings reflect real-world conditions and reaffirm the need for more standardized and robust alignment protocols in SMILE. The small supported differences in refractive predictability, particularly in high or oblique astigmatism, favor toric ICL as the more reproducible approach under current clinical practice.
At one year postoperatively, both SMILE and toric ICL demonstrated excellent refractive stability, with no clinically significant regression or loss of visual acuity. The minor additional reduction in cylinder observed in the ICL group (mean ≈ 0.1 D, p = 0.044) likely reflects subtle long-term axis stabilization rather than true regression.

Comments (0)