Hydroxychloroquine is usually a first-line treatment for SLE [2, 3], but they have opposite effects on CT, even prior to ophthalmological affection. SLE seems to stimulate a thinner choroid [13,14,15], whereas HCQ seems to promote its thickening [9]. As far as we know, this is the first detailed study of the choroid in patients with SLE treated with HCQ. In addition, researchers usually use the ETDRS grid, but its area is smaller than the 6 × 6 mm square that can be analyzed when using the methods we described.
As expected, most of the participants of this cross-sectional study were female, because SLE is more frequent in females. Both eyes were expored because previous studies suggest that CT in right and left eyes is symmetric [16]. Triton DRI OCT is a SS-OCT, so it allows a deep and reliable analysis of the choroid, and its repeatability and reproducibility have been previously proven [17]. Although manual measurements may be adequate, automatic measurements usually show higher rates of reproducibility [18].
Choroidal thickness distribution in healthy controls was similar to previous studies, in which higher values have been reported in central and superior macula [10, 19]. An increase in CT was observed in nasal zones in patients with SLE and HCQ for at least one year. Those regions are exactly where the choroid is thinner in healthy subjects. Although the choroid is usually thicker in central and superior regions, no differences were found. Statistical analysis could not determine whether the variations on CT was due to HCQ or SLE. Due to ethical considerations, we could not enroll a third study group of patients with SLE without treatment, or even a fourth study group of healthy subjects under treatment with HCQ.
It is reasonable that patients with SLE enrolled in previous studies evaluating CT changes were under treatment with HCQ or another drug, but it is not clarified in most of them. This could explain why some authors found a thinning [7, 8], while some others found a thickening [13,14,15]. In case of lupus nephritis, a choroidal thickening takes place, despite not been correlated to the duration of the disease [15]. There is even a previous research whose authors could not detect any variation in CT in SLE patients withouth ophthalmological affection [20]. This could be explained after the small sample size of patients enrolled (20 SLE patients and 20 controls).
On the other hand, HCQ has been associated with thinner CT when being used for different conditions [9, 21], even prior to the development of HCQ retinopathy. In case of HCQ retinopathy, CT gets significantly thinned [21]. Nonetheless, it seems that CT changes can differ depending on the autoimmune disease, that is, some autoimmune diseases may cause a thinning, and some others a thickening in CT [14].
Other authors observed an increase in CT in patients with rheumatoid arthritis, and they explained this increase as a consequence of HCQ [9]. Some other studies evaluated CT variations in patients with SLE under different treatments, but they could not observe an association between HCQ and CT in those receiving HCQ [7]. In contrast with our study, most of these studies analyzed CT using either manual measurements on lineal slabs, or the ETDRS grid obtained with spectral-domain OCT. They did not provide any 3D representation of CT either. Thus, we cannot clearly distinguish whether the variations on CT are due to SLE itself or to its treatment with HCQ.
It should be remarked that increased CT is associated with active phases of SLE, as well as other autoimmune diseases [22]. None of the patients in our study had suffered from an active phase of SLE in the last year, but this might not have been considered in previous studies, and that might be a reason why opposite findings have been found regarding CT.
Arias-Peso et al. showed that the choroid was thicker in patients with SLE and HCQ for less than 5 years of treatment compared with healthy controls in some ETDRS sectors [12]. The main difference with our study is that they included patients with less than one year of treatment. In our study we discarded those patients to verify that HCQ had enough time to show some effects on the choroid. Additionally, they only analyzed ETDRS sectors, so parts of the choroid could not be evaluated.
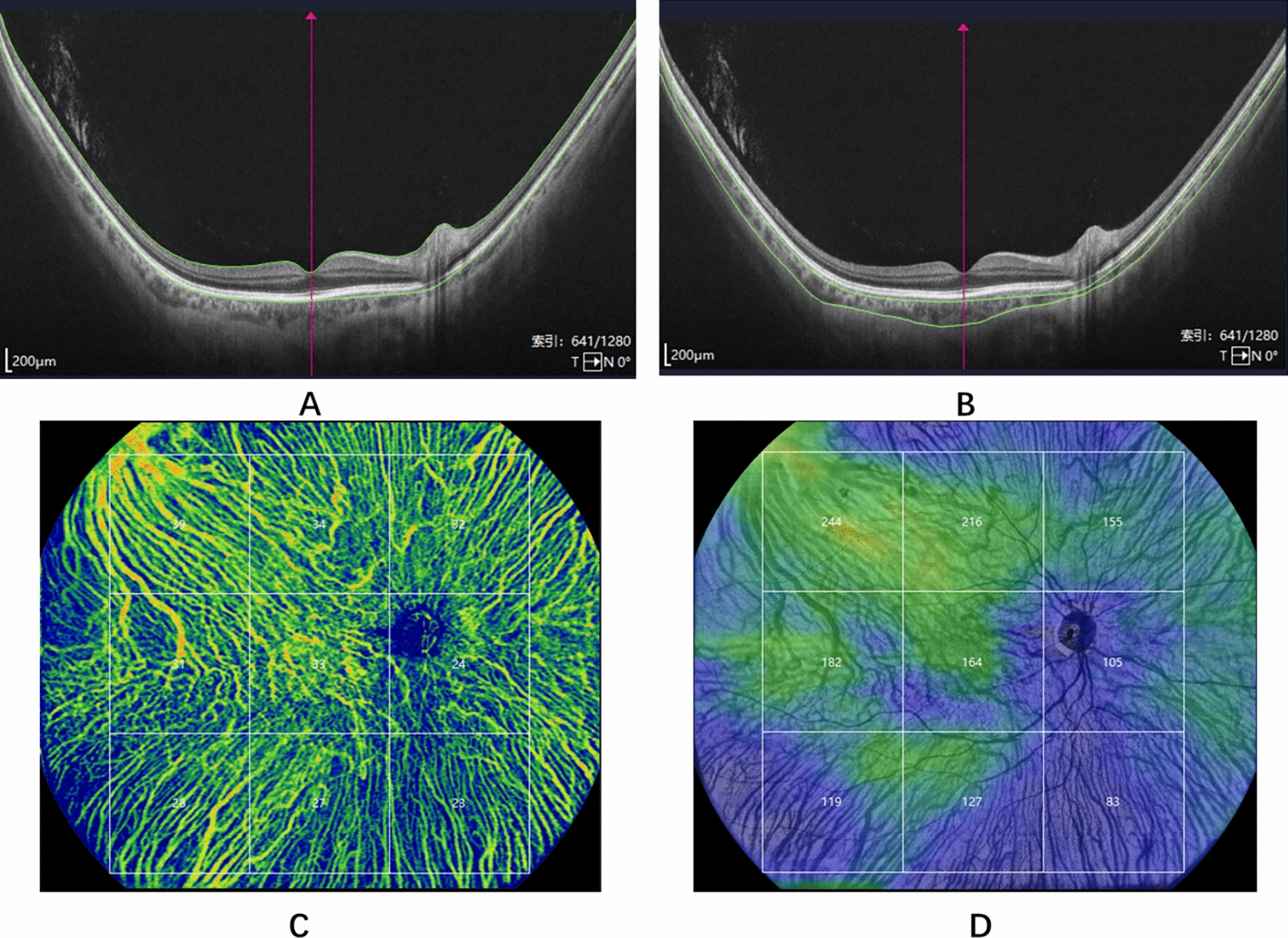
Secondarily, study demonstrated the importance of analyzing the whole choroid in detail. Some parts of the choroid may not be evaluated when using the ETDRS grid. Finally, 3D representations help us detect all these changes in CT at a glance. This is the first time they are provided in patients with SLE or HCQ.
Three-dimension maps have already been published in other ophthalmological disorders, but never in case of SLE or HCQ. Multiple CT maps showed that CT has a different pattern than retina [10, 11, 23]. They also helped understanding CT in patients with high myopia [24], and demonstred local thickening in case of reticular pseudodrusen [25]. Additionally, they may have a role in diagnosing acute central serous corioretinopathy [26].
This study could not associate CT to duration of SLE, nor with duration of HCQ, nor with HCQ dose. Bayuk et al. performed a study comparing CT between SLE patients and healthy volunteers, and nor could they find any association between CT and disease duration, disease activity score, or HCQ dose [27]. Similarly, Braga et al. could not associate variations in CT in patients with lupus nephritis and duration of the disease [15].
Strengths of this study are the sample size and the detailed analysis of the choroid using automatic measurements. Patients older than 55 years were discarded, so cataracts did not interfere with our outcomes. Main limitations are that we could not study the effect of SLE and HCQ separately because HCQ is usually a first-line treatment for SLE [2, 3]. Further research should be performed to confirm our outcomes and it would be of interest to analyze the influence of SLE and that of HCQ on choroid separately.
In conclusion, patients with SLE treated with HCQ for one or more years present higher CT values than healthy subjects. Nasal zones seem to be the most sensitive to these changes, while the other choroidal locations remain similar. However, neither duration of SLE nor duration or dose of HCQ treatment seemed to have any influence on CT. Prospective longitudinal studies should confirm these outcomes.

Comments (0)