This large-scale retrospective cohort study provides important insights into the complications of MIGS in patients with and without DR. This study encompasses patients from several nations and those aged 18 years or older. It is well known that older age (especially 40 years or older) is a significant risk factor for POAG, although younger patients may also be vulnerable in the presence of certain genetic mutations [19, 20]. Nevertheless, our findings suggest that patients with DR undergoing MIGS face increased risks of certain post-operative complications and may have a compounding effect on visual outcomes.
This association can be due to several factors. First, the underlying vascular fragility and tortuosity in patients with DR can lead to weak vasculature that can be further harmed during surgery and contribute to vision loss [21]. Indeed, such vulnerable ocular vessels in DR can be due to chronic hyperglycemia, which damages the endothelium, as well as elevated levels of VEGF in the aqueous humor, which promote neovascularization of further weakened vessels [22, 23]. Second, the compromised retinal function in DR patients can be due to oxidative stress, loss of blood-retinal barrier integrity, and inflammation that could be further impacted by undergoing MIGS [24]. Third, there is a delayed wound-healing process in DR due to the damaged endothelium, which can lead to imbalances in secreted anti-fibrinolytic substances, such as von Willebrand factor and plasminogen activator inhibitor-1, and pro-fibrinolytic substances, such as tissue plasminogen activator [25]. The impaired ability to heal wounds could prevent patients from healing properly from the tissue trauma that can arise from undergoing any procedural intervention.
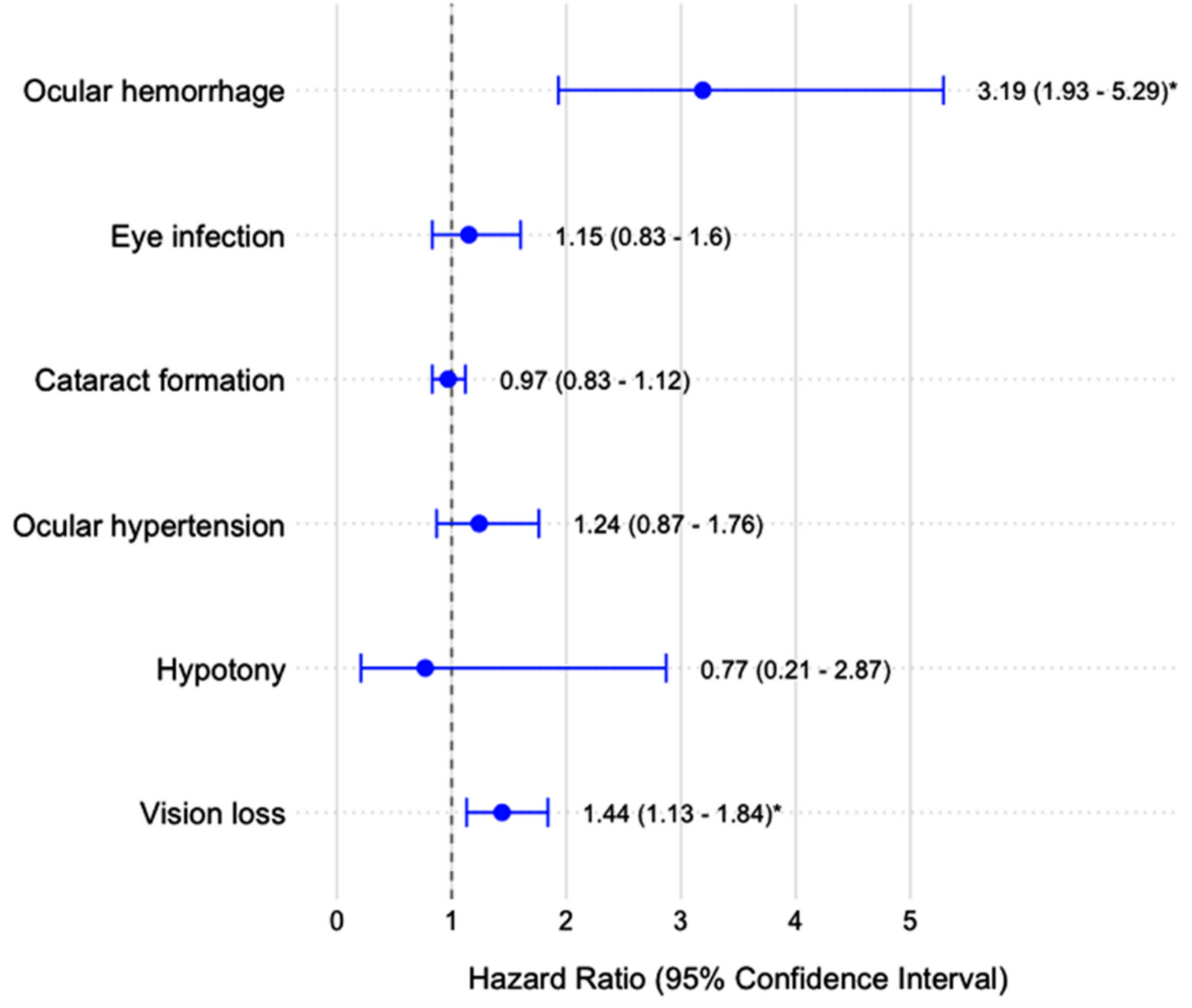
The significantly higher incidence of vision loss in DR patients (32.8% vs. 24.4%, p = 0.005) is a key finding, with DR causing a 44.3% increased risk (HR 1.443, 95% CI 1.13–1.841). Interestingly, several studies support this. Liu et al. examined visual acuity after the Ahmed tube shunt procedure. They noted that one patient who had chronic, uncontrolled DR had a tractional and rhegmatogenous retinal detachment, which led to extensive vision loss within six months after surgery [26]. One possible explanation for this is the ocular hypoperfusion induced during MIGS. Although the literature shows some discrepancies among types of MIGS, a plethora of studies have shown that various MIGS can significantly decrease intraocular pressure and the subsequent need for pressure-lowering drops [27, 28]. Sudden, modest reductions in intraocular pressure can cause retinal ischemia, which may contribute to vision loss [29, 30]. In the current era, instrument sizes for typically extensive surgeries, such as vitrectomies, have become smaller to enable minimally invasive procedures. This allows for more controlled intraocular pressure drops during surgery, potentially mediating the risk of hypoperfusion.
The threefold increase in the risk of any ocular hemorrhage among DR patients (HR 3.194, 95% CI 1.929–5.288) is a strong finding that may also have contributed to the higher risk of vision loss in this patient cohort. This is not surprising given that post-operative hemorrhagic events in general occur in the majority of cases, depending on the specific procedure [31]. We describe ocular hemorrhage as either retinal, conjunctival, vitreous, or choroidal. Although hyphema, or anterior chamber hemorrhage, is a common type of ocular hemorrhage after MIGS, we did not include it as a study outcome. It can be difficult to distinguish post-operative hyphema with or without concomitant clot formation, especially among patients with DR who are more vulnerable to such neovascular complications than those without DR. Indeed, those with clot formation may experience greater post-operative intraocular pressures and higher reoperation rates, prolonging resolution times [32]. Unfortunately, we were unable to assess the incidence of clot formation in the DR and non-DR cohorts, which may limit the utility of assessing hyphema incidence. This is indeed a limitation of a retrospective cohort study utilizing an administrative database, and thus requires future trials to assess the incidence and resolution periods of hyphema with and without clot formation.
Interestingly, our study found lower rates of cataract formation in DR patients at 3 and 6 months post-surgery. One potential explanation lies in the underlying pathophysiology: patients with DR may have aqueous humor with greater antioxidant activity, which may suppress post-operative inflammatory cascades that contribute to early lens opacification [33]. Indeed, given that these were short-term findings, our follow-up window may preferentially under-detect cataract formation in the DR cohort and should be interpreted with caution. Moreover, clinicians may adopt more conservative perioperative steroid prescribing practices in diabetic patients due to a known risk of increased intraocular pressure, thereby mitigating a contributing factor to early cataract formation [34].
The lack of significant differences in rates of hypotony, ocular hypertension, and eye infection between the groups is reassuring, suggesting that MIGS can be performed in DR patients without substantially increasing the risk of these specific complications. This may indicate that the surgical technique itself is equally safe in both groups, but the unique vascular and structural characteristics of DR eyes lead to specific complications.
Our study has several strengths, including its large sample size, the use of propensity score matching to control for confounding, and the assessment of multiple outcomes across different time points. However, it also has limitations inherent to retrospective administrative datasets, such as potential coding errors and a lack of detailed clinical information. This becomes clinically relevant when describing the context of the procedures, such as whether they were isolated or performed in addition to phacoemulsification. Furthermore, we were unable to stratify complications by MIGS type, which may be relevant to clinicians when deciding on specific instruments or treatments. Moreover, we were unable to compare complication risks based on lab value-based DM control.
To our knowledge, this is the first large-scale retrospective cohort study to demonstrate that DR can increase the risk of complications after MIGS, despite its known benefits. This suggests two recommendations. First, controlling DM before any MIGS may reduce this risk. Second, further studies are needed to evaluate the risk of these complications by MIGS type.

Comments (0)