This study suggests that the effect of pupil dilation on spherical IOL power estimation is IOL formula dependent. The Barrett Universal II formula demonstrated an IOL power difference greater than 0.50 D in 28% of eyes. Similarly, the EVO and Cooke formulas showed changes in approximately 25% of cases, while the Kane, Hill-RBF, Hoffer QST, and PEARL-DGS formulas exhibited such changes in around 23% of eyes. These findings indicate that the Kane formula may be less sensitive to dilation-induced biometric variations compared to the Barrett formula. In a similar study, Wang et al. (2018) also reported IOL power differences of ≥ 0.50 D in 48% of eyes using the Haigis and Olsen formulas in a paediatric population. In contrast, Arriola-Villalobos et al. (2013) and Bakbak et al. (2012) using the Lenstar LS, found that only 6 to 9% of eyes demonstrated changes greater than 0.50 D with the SRK/T and Holladay II formulas. Similarly, Can et al. (2016) using the AL-Scan biometer, reported that just 2.8% of eyes showed changes with SRK/T. These interstudy variations may potentially be attributed to differences in patient demographics, the use of age-specific formula such as Olsen, inter-device disagreement, and the varying sensitivity of individual formulas to changes in ocular biometry following dilation.
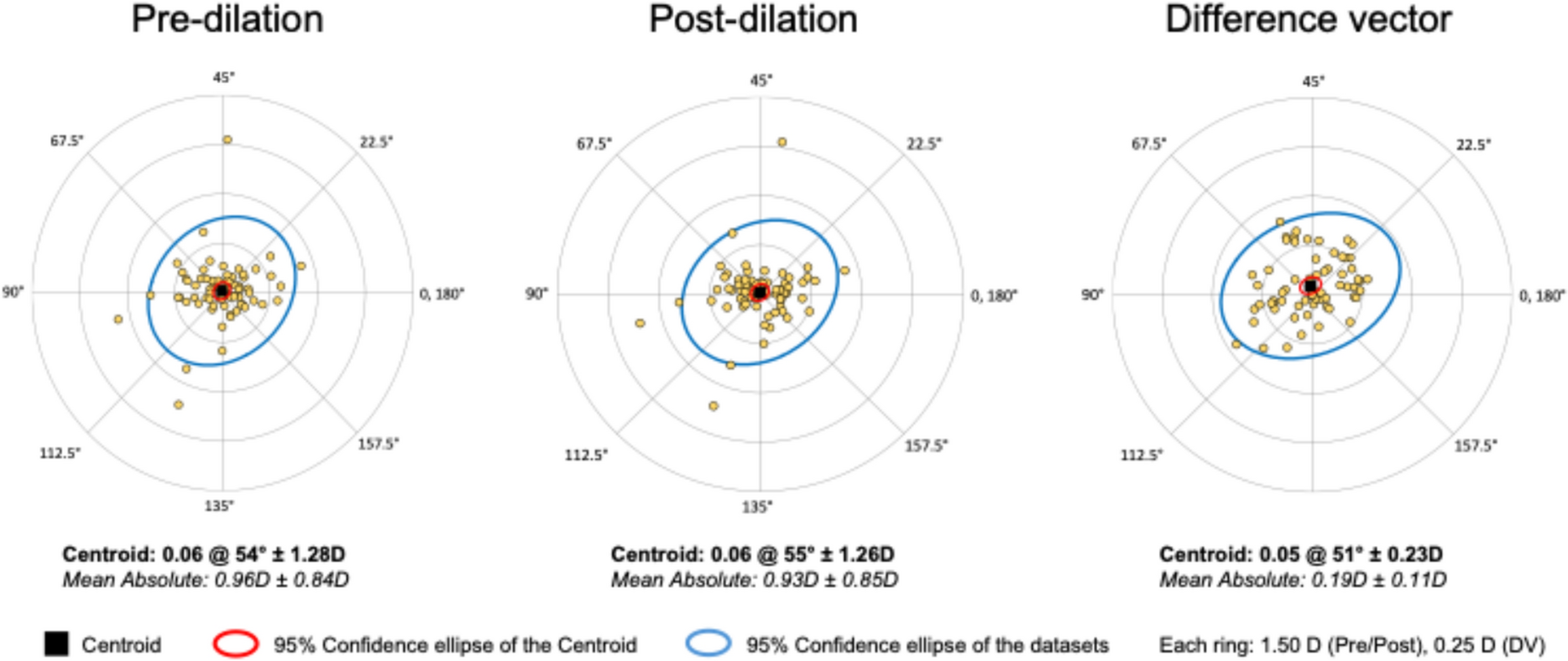
Regarding toric IOL power comparisons, the majority of eyes (> 90%) in our study showed minimal variation (≤ 0.50 D) following dilation, which is consistent with the observed dilation-induced changes in keratometric magnitude (93%). However, axis deviations greater than 10 degrees were observed in a formula-dependent manner. The Hoffer QST formula demonstrated axis variations exceeding 10 degrees in nearly 42% of eyes, whereas the Barrett Universal II, EVO, and Kane formulas showed axis deviations more closely aligned with the changes in keratometric axis induced by dilation, occurring in approximately 24% of eyes. These findings suggest that toric axis estimation is more susceptible to the effects of dilation than toric power estimation, and that the degree of susceptibility is formula dependent.
Although central corneal thickness (CCT) was the only anterior segment parameter that changed significantly in our study, most studies agree that ACD significantly increases post-dilation due to posterior movement of the iris–lens diaphragm and a slight reduction in lens thickness [1,2,3,4,5,6, 8, 11, 14,15,16]. Compared to these studies (mean difference range: from 0.001 mmm to 0.02 mm), we found a greater but non-significant difference in lens thickness, suggesting the variation reflects the changes in posterior movement of the lens. In addition, the absence of statistically significant changes in ACD and LT in our cohort likely reflects the small absolute magnitude of dilation-induced shifts in these parameters, which may lie below the detection threshold once inter-eye correlation and biological variability are accounted for, even though the direction of change is consistent with prior work.
The significant increase in CCT observed here is consistent with physiological responses to mydriasis, as mydriatic agents can induce transient corneal hydration changes or alter epithelial integrity, resulting in small increases in thickness. Importantly, while CCT changed significantly, its influence on IOL power calculation is minimal compared with AL, K, LT and ACD. Therefore, the observed differences in predicted IOL power are more likely attributable to the cumulative effect of small changes across multiple biometric parameters rather than to CCT alone.
These post dilation biometric changes have the potential to influence the prediction of effective lens position (ELP), an essential component in both spherical and toric IOL power calculations. The Hoffer QST formula relies primarily on ACD for ELP estimation and considers only the anterior corneal curvature (K), without incorporating compensation for posterior corneal astigmatism (PCA) [17]. In contrast, the Barrett Universal II formula employs a thick-lens vergence model with empirical refinements and integrates multiple biometric parameters, including ACD, lens thickness (LT), axial length (AL), and white-to-white (WTW), for more accurate ELP prediction. The EVO formula similarly accounts for ACD, LT, and CCT, and is optimized using machine learning. The Kane formula takes a hybrid approach, combining theoretical optics with artificial intelligence, using a comprehensive set of biometric variables to refine both ELP and axis predictions [18]. In addition to ELP modelling, differences in how formulas compensate for PCA further contribute to variability. Unlike Hoffer QST, which uses anterior keratometry alone, Barrett, EVO, and Kane incorporate PCA either through direct modelling or statistical estimation. Taken together, these differences in ELP estimation and PCA compensation likely explain the formula-specific variations in toric axis prediction observed in this study, despite identical keratometric inputs.
Apart from central corneal thickness (CCT) measurements, our study did not find any significant effect of pupil dilation on individual biometric parameters measured with the Anterion biometer. Studies using the IOLMaster, AL-Scan, or Lenstar biometers to assess the effect of dilation have reported inconsistent results across biometric parameters. Our findings regarding keratometric values were consistent with most studies, which have also reported no significant changes, supporting the stability of corneal curvature irrespective of pupil dilation [2,3,4, 6, 11, 14]. Only a few studies, such as those by Wang et al. (2018) and Bakbak et al. (2012) have reported significant changes in keratometric values following pharmacological pupil dilation. Similarly, our study and others examining the effect of dilation on white-to-white (WTW) diameter have resulted in inconsistent findings, suggesting no significant change. In contrast, Wang et al.[1] and Xi et al.[7] reported significant changes in WTW diameter, particularly in highly myopic eyes. It has been hypothesised that pharmacological dilation may alter ciliary muscle tone, indirectly affecting the scleral spur and peripheral cornea. Additionally, the shift in the image reference edge, from a lighter to a darker iris–limbus border becoming more prominent under dilation could contribute to inconsistent WTW measurements.[7]Our findings, along with other studies, show no significant change in axial length (AL) after pharmacological dilation. Although Wang et al. (2018) and Xi et al. (2022) observed small differences of about 0.01 mm, these variations are unlikely to affect intraocular lens (IOL) power calculations due to their minimal magnitude.
Limitations of our study include the relatively small sample size, though adequately powered for detecting mean differences in biometric variables, and the use of a single IOL model (ZCB00) which may restrict the generalisability of our findings to other IOL design. Although our study did not find a significant difference in biometric measurements pre- and post-dilation, this result could be influenced by the precision and repeatability characteristics of the Anterion device itself. Therefore, future studies should include multiple biometers to better understand the interaction between pupil dilation and instrument-specific measurement differences. Additionally, we did not assess postoperative refractive outcomes. As a result, we are unable to correlate any changes in preoperative biometry due to dilation with the eventual refractive success of the surgery.
In addition, some cataracts may become more clinically apparent after pharmacologic dilation, our study did not categorise patients based on cataract visibility pre- and post-dilation; therefore, we were unable to assess whether such eyes were more likely to demonstrate larger (> 0.50 D) differences in predicted IOL power. This represents an interesting consideration for future studies.
Although no baseline biometric parameters were significantly associated with clinically meaningful (≥ 0.50 D) IOL power shifts following dilation, a trend toward greater susceptibility in eyes with thicker crystalline lenses was observed. This finding may reflect subtle lens‑related biometric changes during dilation that are not fully captured by current models. Future studies with larger sample sizes or multivariable modeling may help identify specific biometric profiles at greater risk for dilation‑induced power prediction variability and refine formula performance in such eyes.
Despite the lack of postoperative refractive outcomes, our findings provide important insights into ANTERION measurements under dilated conditions. This is particularly relevant for understanding how instrument-specific factors may influence biometric measurements, especially given the known inter-device variability reported in the literature. Even small shifts in biometry can affect IOL selection, which is critical in eyes with borderline values or when planning premium IOL implantation. While previous studies have assessed dilation effects using other biometers, our study is among the first to systematically evaluate these changes using the ANTERION, including their impact on predicted IOL power. Future studies incorporating postoperative refractive outcomes and comparisons across multiple biometers are needed to confirm the clinical significance of these observations.
In conclusion, pharmacological pupil dilation had minimal effect on most ocular biometric parameters measured using the Anterion biometer. However, clinically significant changes in spherical IOL power predictions were observed in approximately 25% of cases, depending on the formula used. Toric power predictions showed clinically significant variation in only a minority of eyes, while toric axis predictions demonstrated formula-specific variability, with clinically significant deviations (> 10°) noted in a substantial proportion of cases, particularly with the Hoffer QST formula. To minimise dilation‑related error in IOL calculations, biometric measurements should preferentially be obtained under normal, undilated physiological conditions; however, surgeons may also consider patient‑specific visual demands (e.g. predominantly bright versus low‑light working conditions) during preoperative counselling, and discuss whether optimisation for the undilated state alone is appropriate or whether the potential impact of the dilated state on visual performance should also be taken into account.

Comments (0)