The present study, based on national register-based data, comprehensively analysed the prevalence of overall potentially clinically significant DDIs among multimorbid older Swedish adults (≥ 65 years) with AF who were prescribed ≥ 2 drugs. Additionally, the study assessed potential correlates of overall DDIs, prevalent DDI categories and their association with adverse clinical outcomes over a two-year period. In this study population, 37.5% of the individuals had ≥ 1 DDI. Moreover, the association between demographic variables and DDIs varied depending on the type of DDI analysed, with sex, age, and civil status identified as the strongest and most consistent correlates. Finally, a higher hazard of adverse clinical outcomes was observed depending on the type of DDI assessed.
Prevalence of Potentially Clinically Significant DDIs
Our study found a significantly lower prevalence (8.2%) of DDIs involving DOACs compared to the few previous studies available [14, 33], with the most common interactions occurring with SSRIs, tetracyclic antidepressants, CYP3A4 inhibitors, and P-gp inhibitors. Most existing studies on potentially clinically significant DDIs in older adults with AF have focused on (D)OAC-related interactions, reporting prevalence rates ranging from 26.7% to 59% [14, 33]. The Swedish National Board of Health and Welfare implemented in 2012 a regulation requiring healthcare providers to offer medication reviews to all patients aged 75 years or older using ≥ 5 drugs [34], which might have contributed to the lower observed prevalence of DDIs with DOACs in our study. A study assessing the overall prevalence of DDIs in AF patients admitted to the emergency department reported a prevalence of 19%, with CV drugs being most frequently implicated [35]. This prevalence is notably lower than the 37.5% identified in the present study, which predominantly involved community-dwelling older adults suffering from multimorbidity. The discrepancies reflect differences in study settings and target populations.
Similar heterogeneity between studies has been observed in the general population (non-AF specific) [3, 11, 32, 36,37,38]. Comparing DDI prevalence across studies is challenging due to variability in the DDIs examined and the tools used for DDI identification [39]. Three studies used the same explicit international consensus list of potentially clinically significant DDIs as in our study and reported a prevalence ranging from 46% to 54% in the general population aged ≥ 65 years (non-AF specific) [3, 11, 40]. The most frequent interactions identified included combinations of potassium-regulating medications, OACs with antiplatelet drugs, concomitant use of ≥ 3 CNS-acting drugs and SSRI with diuretics [3, 11, 40]. Similar DDIs were observed in our study population, along with additional interactions such as digoxin-diuretic combinations, SSRI-serotonergic, and DOAC-tetracyclic antidepressant interactions, as well as statins with amlodipine. Furthermore, similar drug classes, particularly CNS and CV drugs, were also implicated in potentially inappropriate prescribing and omissions respectively [27]. This highlights the need for increased vigilance and more thorough medication reviews, with particular attention to the appropriate prescribing of these drug classes.
Interestingly, when OTC medication use was considered, analgesics, mainly paracetamol and ibuprofen were frequently identified, interacting particularly with aspirin or amitriptyline [38]. OTC medications have been reported to be involved in DDIs leading to hospitalisation [38]. Since OTC medications are not recorded in the registers, we could not provide a full overview of potential drug combination risks.
Association of Potentially Clinically Significant DDIs and Socio-demographic Variables
Previous studies have reported inconsistent associations between demographic variables and potentially clinically significant DDIs. For example, while most studies reported lower odds of DDIs among males [37, 41], in line with our results, Guthrie et al. 2015 identified higher odds [32]. Discrepancies also exist regarding the role of age [7, 11, 32, 37, 41]. These discrepancies between studies can be attributed to several factors. First, the type of DDIs examined varied: as demonstrated in our study, when specific DDIs are examined, higher odds are observed whereas when grouped into broader drug categories lower odds are obtained. Second, the tools used to identify DDIs differed across studies (e.g. British National Formulary, Lexi-interact Module, Micromedex) [32, 37, 41]. Third, variations in the relationship between demographic variables and DDIs, may stem from differences in the clinical profile of the study populations and the covariates adjusted for. While our study focused on adults aged 65 years and older with multimorbidity, two other studies included the complete population [32, 41]. Additionally, some studies adjusted for factors such as place of residence (care home vs. community-dwelling), self-medication, number of prescribers and number of pharmacies per person [32, 37, 41].
Interestingly, when focusing on DOACs and the use of ≥ 2 potassium sparing drugs, lower odds of DDIs were observed in older age groups. This suggests that clinicians may be more cautious in prescribing and, consequently, more diligent in avoiding DDIs involving (D)OACs in older adults [27]. Chronic diseases also play an important role after adjusting for polypharmacy. For example, individuals with CV diseases (e.g., AF, heart failure) or CNS conditions (e.g., depression) showed higher odds of DDIs, even after adjusting for polypharmacy. Conversely, those with chronic hepatic failure exhibited reduced odds [11], while musculoskeletal conditions or cancer were not significantly associated [38]. A parallel can be drawn with our ten most prevalent DDIs, which involved SSRI and diuretic agents.
Finally, it is important to note that while some associations were statistically significant, they may not necessarily be clinically relevant, given the study’s substantial population size. The strength of the OR should be considered in this context. These findings highlight the complexity of DDI patterns, and the need to contextualise results within the characteristics of the study population.
Association of Potentially Clinically Significant DDIs and Adverse Clinical Outcomes
DDIs were associated with adverse clinical outcomes across various categories, either as specific interactions or through broader DDI medication classes. Most studies in the literature have primarily focused on the association between DDIs involving DOACs and bleeding. While a DDI might not directly cause death, it could function as an intermediate factor or trigger the underlying cause.
Overall, our findings indicate that patients with DDIs, especially those involving diuretics, digoxin, DOAC and SSRIs were associated with a higher hazard of hospitalisation. This might be in part attributable to ADRs. Previous studies have demonstrated that DDIs in older adults are associated with an increased risk of ADR-related hospitalisations and a longer median hospital stay [42, 43]. Particularly CV drugs – such as heart glycosides, OACs, diuretics, NSAIDs, and psychotropic drugs – are frequently involved. The most common ADR resulting from DDIs include gastrointestinal bleeding, cardiac rhythm disturbances, nephrotoxicity and electrolyte imbalances [43,44,45,46]. In our study population, individuals using ≥ 3 CNS-acting agents initially exhibited a higher hazard of CV hospitalisation in the unadjusted analysis; however, after adjusting for confounders, this association reversed to a lower hazard in the multivariable model (HR 0.96 [0.92–0.99]), compared to those without a DDI. Although this reversal is statistically significant, its modest effect size may suggest limited clinical relevance or a statistical quirk —especially considering the concurrent findings of a 66% increased hazard of death, a 16% higher hazard of overall hospitalisation, and a 17% increased hazard of stroke.
No statistically significant association was observed when using a composite bleeding outcome. However, sensitivity analyses stratifying by bleeding type revealed a statistically significant increased hazard of gastrointestinal bleeding, but not for intracranial haemorrhage. These findings align with prior studies in older adults with AF [14, 47,48,49]. In one study, an association with intracranial haemorrhage was detected only for specific interactions, namely DOAC-SSRI and DOAC-corticosteroids [14] or pharmacodynamic DDIs involving rivaroxaban [49], compared to adults without a DDI. Similarly, DDIs involving apixaban and rivaroxaban were associated with gastrointestinal bleeding compared to those without a DDI [17, 49]. Potentially inappropriate dosing of DOACs may also contribute to an increased bleeding hazard. However, the literature presents inconsistent results regarding the association between inappropriate dosing and bleeding hazard [50,51,52,53,54,55,56]. Additionally, as previously mentioned, Swedish regulations on targeted medication reviews [34] may have contributed to appropriate prescribing, potentially reducing the bleeding risk.
Regarding stroke, our findings confirmed a higher hazard in patients with DDIs, consistent with other studies [47, 57]. This association is likely driven by interactions that reduce the effectiveness of oral anticoagulants, particularly DOACs. Certain drugs, such as carbamazepine or rifampicin, can accelerate the metabolism of DOACs, lowering their blood concentrations and thereby reducing protection against thromboembolic events such as cerebral infarction [29, 58, 59]. In addition, some DDIs may lead to anticoagulant dose reductions or discontinuation due to bleeding concerns, which can further increase the risk of stroke.
For falls, we observed that DDIs involving CNS medications were strongly associated with an increased hazard. This could be attributed to the use of ≥ 3 CNS-acting medications (opioids, hypnosedatives, barbiturates, antipsychotics, antidepressants and antiepileptics), which are due to enhanced sedative effects and orthostatic hypotension, known as fall risk increasing drugs and are a target for deprescribing [60]. Interestingly, those using ≥ 2 potassium sparing medications were associated with a lower hazard of falls compared to those without a DDI. While the clinical relevance of this finding is unclear, it may be explained by unmeasured confounders or differences in patient characteristics, which were beyond the scope of this study. Factors such as medication adherence, self-monitoring, and genetic polymorphisms might underlie the observed risks and should be explored in future studies [40]. Whether a DDI results in harm often depends on the patient’s clinical profile among other variables. Managing patients with complex conditions requires vigilant monitoring [40] and multidisciplinary consultation to determine the best approach [17, 61].
Finally, in the secondary analysis, the two-year population attributable fractions for DOAC-related DDIs were small for overall and CV mortality, overall and CV hospitalisation, and were not statistically significant for stroke, bleeding, or falls. These findings suggest that, although DOAC-related DDIs were associated with higher hazards, the population-level burden attributable to DOAC-related DDIs over two years was limited. This dual perspective may aid clinicians by highlighting that individual patient management remains important even if the overall public health impact is limited. However, these estimates should be interpreted considering possible residual confounding and potential treatment changes during follow-up.
Clinical Implications
This study is timely given the increasing global healthcare burden of AF and multimorbidity, as well as the increase in polypharmacy due to global ageing. Furthermore, it aligns with World Health Organisation’s medication safety priority, emphasising the need to address polypharmacy and DDIs as critical components of global patient safety.
Our findings underscore the importance of tailored approaches in managing older adults with complex health profiles, where identifying high-risk groups is essential for preventive strategies and effective clinical management [37]. The Atrial fibrillation Better Care pathway is an integrated, multidisciplinary and holistic care approach aimed at improving AF management based on three core components: (A) stroke prevention, (B) better symptom management and (C) cardiovascular risk factors and comorbidities management [62]. Targeting potentially inappropriate prescribing patterns could improve therapeutic management and would align with concept C, comorbidity management. This additional focus would support a more integrated, multidisciplinary approach.
Integrated, personalised care remains vital to addressing the complexities of older adults’ medication regimens and improving their health outcomes. Future research should prioritise several key areas. First, mechanistic studies are essential to explore the protective effects of potassium sparing drugs on falls, focusing on their potential interactions with cardiovascular function or fluid balance. In addition, prospective cohort studies or randomised controlled trials are recommended to assess whether deprescribing CNS drugs can reduce adverse clinical outcomes in older adults with AF. Furthermore, qualitative research is crucial to understand prescribing behaviours, particularly to investigate why certain DDIs, such as those involving DOACs, occur less frequently in older adults. Research should also address the discrepancy in bleeding risks associated with DOAC-related DDIs, considering potential covariates such as stricter prescribing protocols or enhanced patient education efforts, which could contribute to reduced bleeding risks in specific cohorts.
Finally, it is important to engage policymakers in supporting initiatives such as mandatory DDI training for prescribers and securing funding for medication review programs aimed at high-risk populations. Additionally, fostering dialogue between pharmaceutical companies and healthcare providers is crucial to address gaps in drug labelling that fail to adequately warn about clinically significant DDIs. Collaboration with patient advocacy groups is also essential to raise awareness of DDI risks, particularly among older adults who manage their own medications.
Limitations
This study has several limitations that should be acknowledged. First, we did not account for drug-disease or drug-food interactions, which are also important contributors to adverse clinical outcomes and may mediate the relationship between DDIs and health outcomes. Second, we were unable to include established risk scores for stroke and bleeding. This may have limited our ability to fully adjust for baseline risk and could contribute to residual confounding. Similarly, residual confounding by indication may persist, as we were unable to adjust for clinical complexity beyond polypharmacy, which was used as a proxy for disease burden. Individuals with poor health status are more prone to adverse clinical outcomes, which could partially explain the observed associations between DDIs and outcomes.
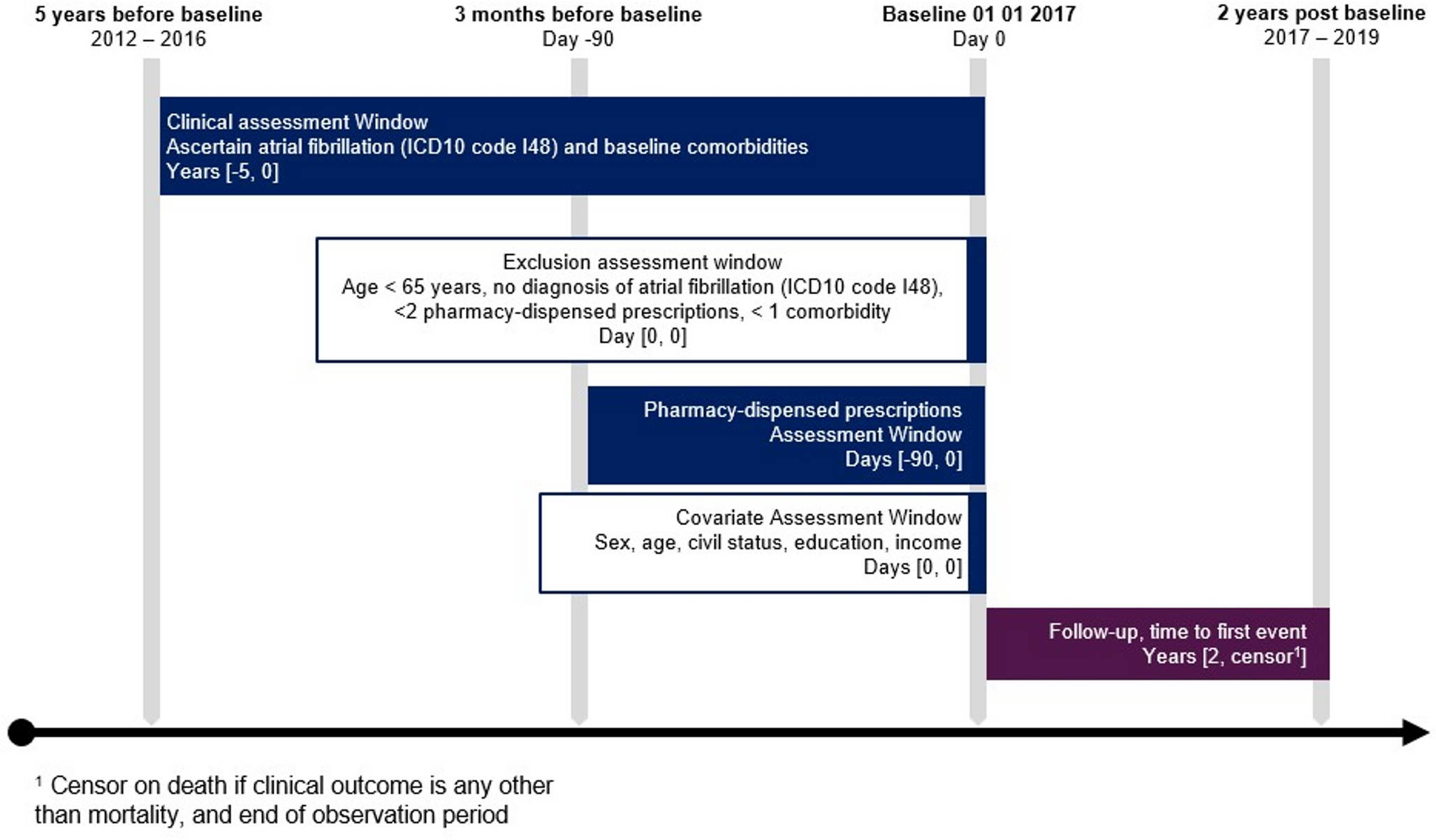
Moreover, residual confounding may arise from not adjusting for AF subtype in the Cox regression analyses. Adults with persistent/permanent AF are typically older, have a higher disease burden, and are more likely to receive OACs [63, 64]. In non-anticoagulated cohorts a higher risk of stroke and mortality was identified in those with persistent/permanent AF compared to those with paroxysmal AF [65, 66]. In contrast, stroke risk may be comparable across AF subtypes in the anticoagulated population [67]. If DOAC use, and consequently the likelihood of DOAC-related DDIs is more common in persistent/permanent AF, part of the observed increased hazard could reflect AF duration rather than the DDI itself, despite adjustment for age and polypharmacy. A related limitation concerns disease duration and long-term medication history. Individuals diagnosed with AF and other chronic conditions are treated over a continuous period, during which their medication regimens evolve. Patients with a longer disease duration may therefore have experienced different or more complex treatment trajectories than those recently diagnosed. By extracting all pharmacy-dispensed prescriptions in the 90 days prior to baseline, it was possible to identify most clinically relevant DDIs present at baseline. However, drug exposures prior to this time frame were not collected and might include potentially clinically significant DDIs that could influence subsequent risks of adverse clinical outcomes. In addition, individuals who experienced severe consequences of earlier DDIs may not survive or remain eligible until the start of follow-up, resulting in left-truncation bias. This limitation is particularly relevant for chronic conditions, including AF, where treatment trajectories change over time.
Additionally, due to the use of register data, we cannot confirm whether patients used these medications concomitantly or adhered to their prescribed treatments. While robust, register-based data cannot capture additional nuances like intentional prescribing of DDIs for therapeutic benefit, or patient behaviours that mitigate DDI risks. Given variations in healthcare systems and prescribing practices, our findings from Swedish national registers may have limited generalisability to countries with different medication review policies or prescribing habits. Dosing information was not included in our analysis, which may limit our ability to fully assess the association of DDIs with adverse clinical outcomes.
The large sample size, while a strength, may lead to statistically significant findings that lack clinical relevance. To aid interpretation, incidence rates for adverse clinical outcomes were reported. Another limitation is the inability to evaluate the appropriateness of DDIs. Assessing whether a DDI is appropriate requires detailed, case-specific information. While potential clinically significant DDIs indicate risk, the actual occurrence of harmful DDIs is typically lower [31]. This distinction is important when interpreting our findings. Furthermore, we did not evaluate the association between DDIs and adverse drug events. However this has been addressed in previous research. Also, OTC medications and herbal supplements were excluded, which may underestimate the true prevalence of DDIs, particularly interactions involving herbal supplements (e.g., St. John’s wort).


Comments (0)