
Remember me
Among 661 patients included with an alternative diagnosis, median age was 66 years (range: 2–91) and 335 patients (51%) were male. CNS was the site of predominant involvement in 397 (60%), PerNS in 215 (33%), and extra-NS in 49 (7%).
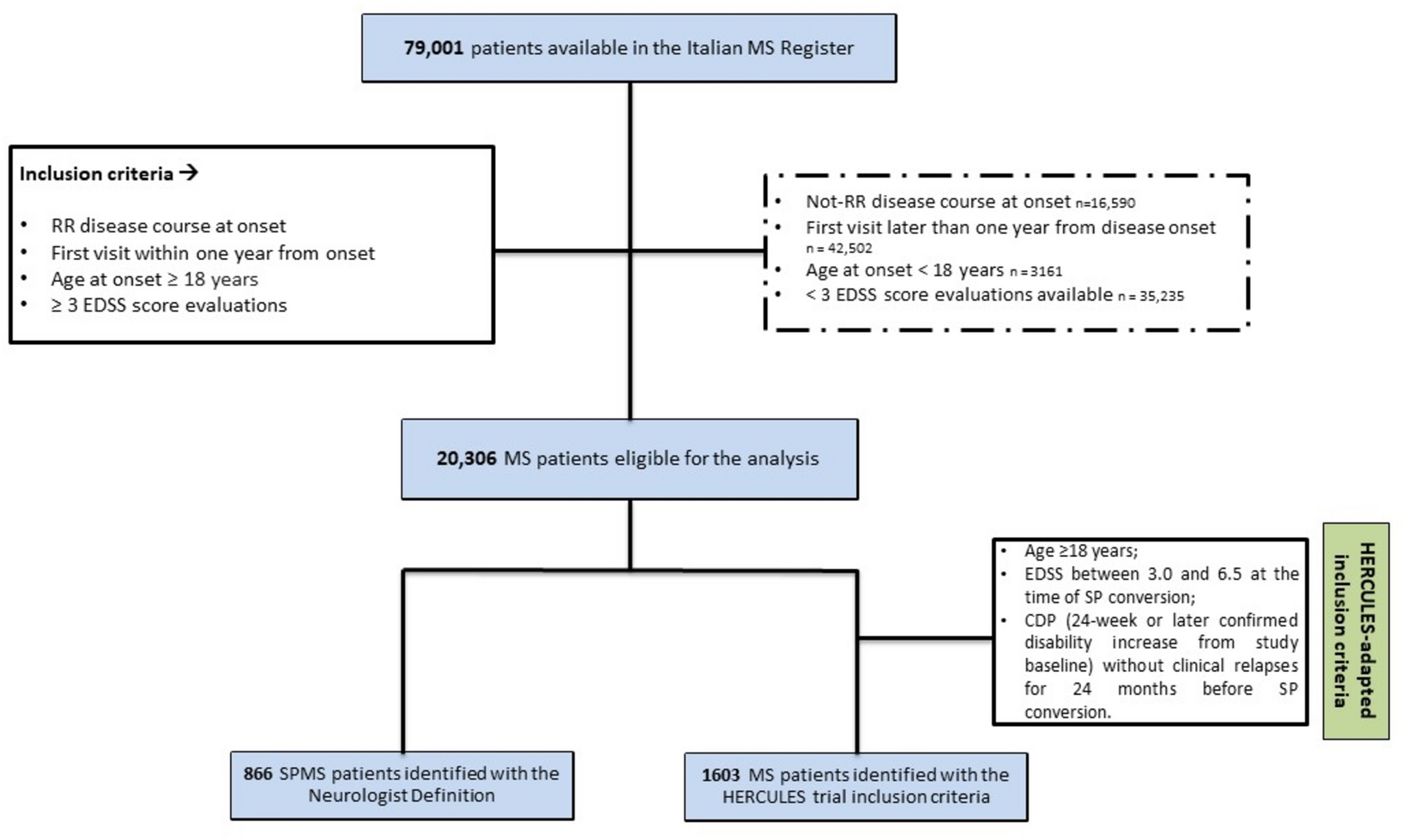
Alternative diagnoses with central nervous system involvementDuring the study period, an alternative diagnosis was established in 269/397 patients with CNS involvement (68%), while it remained unknown in 128 (32%; e.g., epilepsy of unknown etiology). When a final diagnosis was reached (n = 269), the most frequent etiologies were, in order of frequency: degenerative 97 (36%), autoimmune 47 (17%), vascular 37 (14%), neoplastic 26 (10%), infectious 21 (8%), psychiatric 13 (5%), and metabolic 10 (4%), followed by other less frequent diagnoses in 18 (7%) (Fig. 1).I have uploaded a new version of Figure 1 identical to the previous one, with slightly larger labels to improve readability.
Fig. 1
Alternative neurological diagnoses encountered (“better explanations”) during PNS workup. Note that the graphs refer only to cases where a final diagnosis was established (n = 269 for patients with central nervous system manifestations and n = 112 for those with a peripheral nervous system presentation)
Among neurodegenerative conditions tested for PNS Abs (n = 97), the most common diseases were represented by degenerative dementias (n = 32, 33%), motor neuron diseases (MND) (n = 31, 32%), and degenerative movement disorders (n = 24, 28%). In the group of degenerative dementias (n = 32), detailed diagnoses were reached in 18 cases (56%), while in 14 (44%), the follow-up and cerebrospinal fluid (CSF) biomarkers permitted only a diagnosis of unspecified degenerative dementia. Dementia diagnoses included Alzheimer’s disease (AD) (n = 5), mixed dementia (vascular and AD) (n = 3), frontotemporal dementia (n = 3), Lewy body dementia (n = 3), Creutzfeldt–Jakob disease (CJD) (n = 3), and primary progressive aphasia (n = 1).
In the group of MND (n = 31), the majority of the cases (n = 22, 71%) were atypical for classic amyotrophic lateral sclerosis (ALS) and the clinical features that led to neuronal Ab testing were the presence of increased CSF protein content (n = 5), young age at onset (< 50 years) (n = 4), concomitant sensory disturbances (n = 4), infrequent clinical variants (flail arm syndrome n = 2, Hirayama disease n = 1, primary lateral sclerosis n = 1), presence of a concomitant systemic tumor (n = 3), or presence of associated cognitive disturbances at onset (n = 2).
Patients with degenerative movement disorders (n = 24) included cases with atypical parkinsonism (n = 11, including 4 patients with multiple system atrophy [MSA]), idiopathic Parkinson’s disease (PD) (n = 9), chorea (n = 3, including 2 cases of Huntington’s disease), and pure autonomic failure (PAF) (n = 1). The most frequent reason for neuronal Ab testing in patients with movement disorders was the detection of a systemic tumor (n = 6, 25%), followed by the presence of autonomic dysfunction (n = 5, 21%).
Patients with an autoimmune etiology (n = 47) comprised those with non-paraneoplastic AE (n = 18, 38%), multiple sclerosis (MS) (n = 11, 23%), myelitis (n = 8, 17%), optic neuritis (n = 4, 8%), acute disseminated encephalomyelitis (ADEM) (n = 3, 6%), and less common diseases (cerebellitis, Sydenham chorea, and autoimmune hemichorea in 1 each). A subgroup of AE cases harbored neuronal surface Abs, including 4 patients with LGI1-Abs and 2 with CASPR2-Abs, all 6 without an associated tumor. The presence of cancer was detected in a minority of the other patients with autoimmune diseases mimicking PNS (n = 4, 9%).
Vascular disorders (n = 37) included ischemic stroke (n = 17, 46%), vasculitis (n = 10, 27%), subcortical vascular encephalopathy (n = 5, 14%), spinal infarction (n = 3, 8%), and hemorrhagic stroke (n = 2, 5%). A tumor was detected in 6 of them (16%). Among the 10 cases of vasculitis, 6 were primary angiitis of the central nervous system (PACNS), while 4 were systemic vasculitis with involvement of the CNS (Churg–Strauss syndrome, Behçet disease, anti-neutrophil cytoplasmic antibodies (ANCA)-associated vasculitis, and leukocytoclastic vasculitis in 1 each).
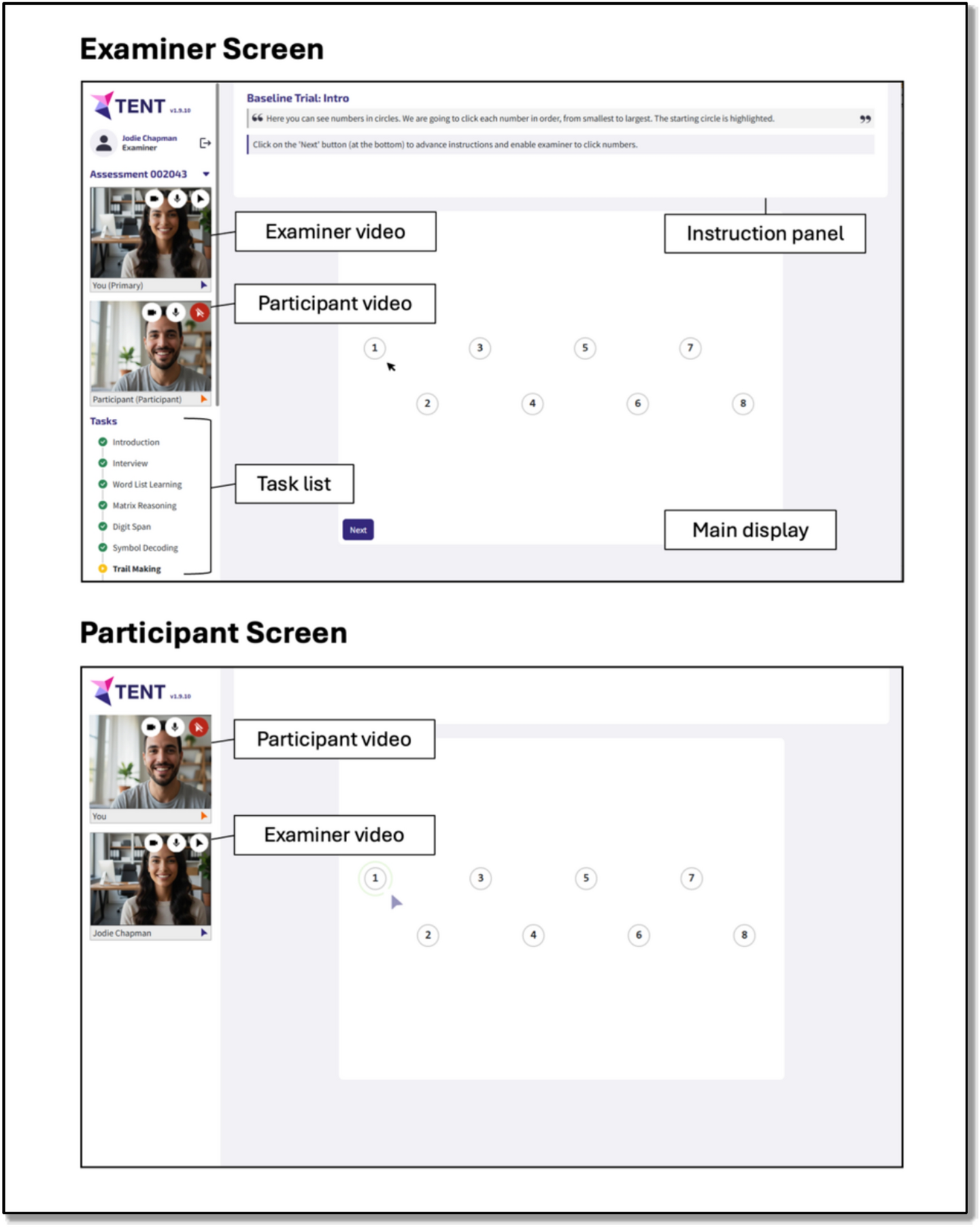
Neoplastic disorders (n = 26) included metastasis from systemic cancer (n = 12, 46%), primary brain tumors (n = 10, 38%), and carcinomatous meningitis (n = 4, 15%). Imaging examples of patients with an alternative neoplastic diagnosis are presented in Fig. 2.
Fig. 2
Imaging examples of patients who were initially thought to have PNS but later had an alternative neoplastic diagnosis. A and B Two distinct cases of leptomeningeal carcinomatosis are shown. In case A, axial FLAIR images demonstrated moderate dilation of the lateral ventricles, associated with periventricular hyperintensities, particularly at the level of the frontal horns. Post-gadolinium SE T1-weighted images revealed enhancement along the vermis and cerebellar sulci. In case B, a bright signal along the cerebellar sulci was seen on axial FLAIR images, while diffuse leptomeningeal enhancement was observed on coronal post-gadolinium SE T1-weighted images. C Multiple hyperintense lesions on T2-weighted and FLAIR images involved both the cortex and white matter of the left frontal lobe and right temporal lobe. No contrast enhancement was seen on post-gadolinium SE T1-weighted images; however, perfusion evaluation revealed a significant increase in relative cerebral blood volume (rCBV) in the same areas. The patient was diagnosed with a biopsy-proven multifocal glioblastoma. D Sagittal TSE, Short TI Inversion Recovery (STIR) T2-weighted, post-gadolinium TSE T1-weighted, and axial Gradient Echo (GE) T2-weighted images showed diffuse thickening of the cauda equina nerve roots. Mild enhancement was noted on T1-weighted images. The spinal canal diameter was normal, and no focal disk herniations were detected. The patient had non-Hodgkin lymphoma (NHL) and was diagnosed with neurolymphomatosis
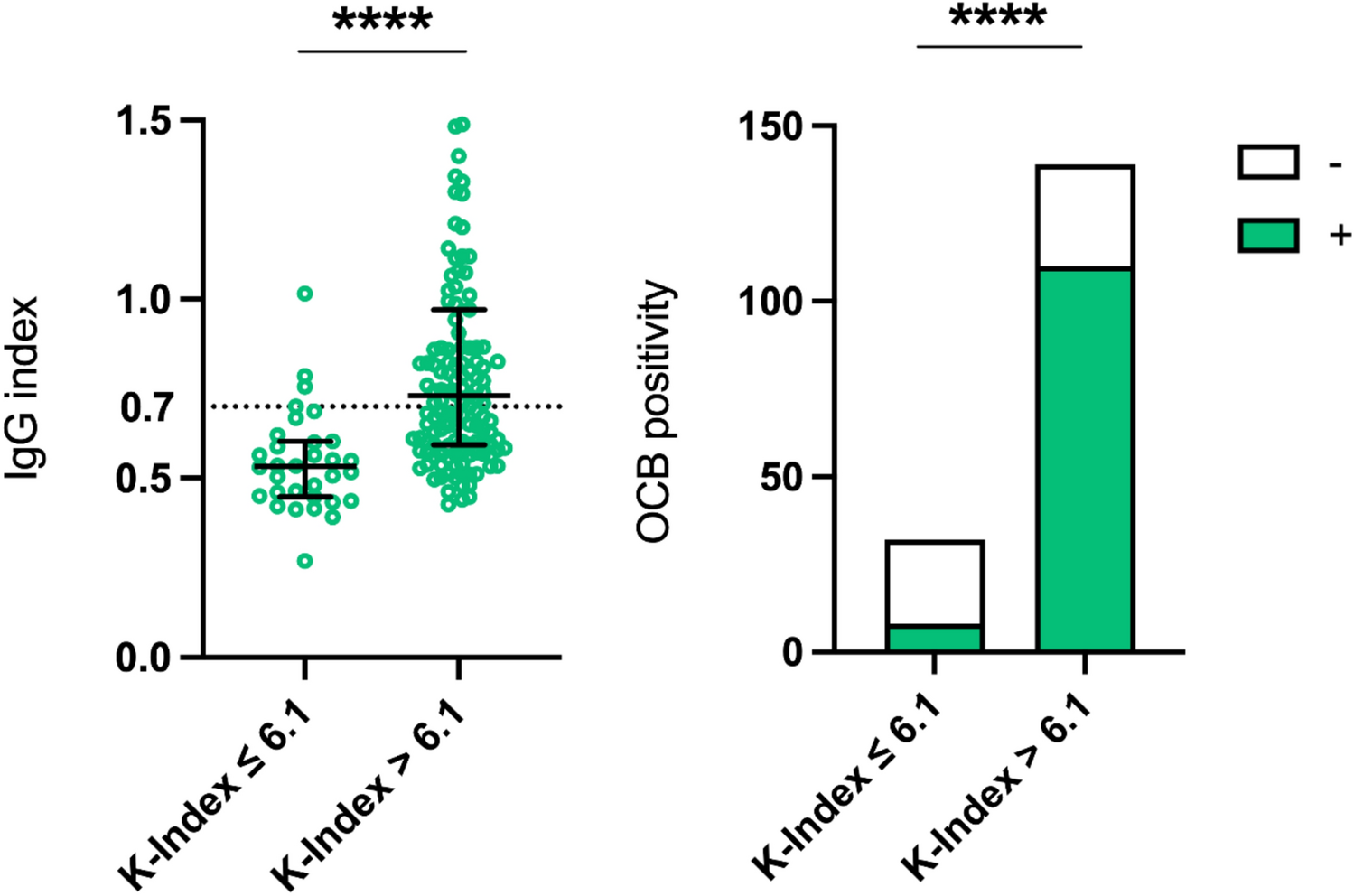
Infectious diseases (n = 21) were infectious encephalitis or meningoencephalitis (n = 16, 76%), infectious myelitis (n = 2, 10%), septic encephalopathies (n = 2, 10%), and infectious (West Nile virus-associated) optic neuropathy (n = 1, 5%). Imaging examples of patients who were initially thought to have PNS but later had an alternative autoimmune or infectious diagnosis are presented in Fig. 3.
Fig. 3
Imaging examples of patients who were initially thought to have PNS but later had an alternative autoimmune or infectious diagnosis. A Axial Fluid Attenuated Inversion Recovery (FLAIR) and coronal multiplanar reconstruction of volumetric Turbo Spin Echo (TSE) T2-weighted sequence showing multifocal, asymmetric, and bilateral hyperintensities involving deep and subcortical white matter of both cerebral hemispheres. The lesions were sparing the cortex and involved U-fibers. These findings were consistent with a classic form of progressive multifocal leukoencephalopathy (PML) which was later confirmed by JCV detection on cerebrospinal fluid. B Axial TSE T2-weighted and coronal FLAIR images demonstrating a hyperintense lesion extending from periventricular white matter to the corona radiata. On post-gadolinium Spin Echo (SE) T1-weighted images a focal, linear enhancement in the same area was present. Intense pachymeningeal enhancement and a dural nodule were also noted. All these findings were suggestive of central nervous system vasculitis. A diagnosis of primary angiitis of the central nervous system (PACNS) was made. C Sagittal TSE T2-weighted of cervical spine and axial FLAIR images showing a large T2-weighted hyperintensity lesion involving the cervical spinal cord for more than two metameres and a focal hyperintensity on the posterior side of the medulla on the left, consistent with a final diagnosis of acute disseminated encephalomyelitis (ADEM). D Multiple hyperintense T2-weighted focal lesions showing diffusion restriction [high signal on apparent diffusion coefficient (ADC) map] on both cerebellar hemispheres. A mild enhancement along cerebellar folia was seen. The patient had an infectious cerebellitis due to Coxsackie virus
Patients with psychiatric diseases (n = 13) comprised functional neurological disorders (n = 5, 38%), primary psychosis (n = 4, 31%), or other psychiatric diseases (n = 4, 31%).
Toxic and metabolic disorders (n = 19) included cases of vitamin deficiency with neurological involvement (n = 6, 32%), alcohol-related CNS disorders (n = 4, 21%), neuroleptic side-effects (n = 2, 10%), and other less frequent toxicities (drug-related optic neuritis, radiation toxicity, and opioids overdose in 1 each) or metabolic disorders (multifactorial in 2, and hyponatremic encephalopathy and hepatic encephalopathy in 1 each).
Alternative diagnoses with peripheral nervous system involvementDuring the study period, the etiology was identified in 112/215 patients with PerNS involvement (52%), while in 103 (48%), it remained unknown. The most frequent etiologies were, in order of frequency: autoimmune 51 (45%), toxic-metabolic 40 (36%), and vascular 11 (10%), followed by other less frequent categories in 10 (9%) (Fig. 1).
Among disorders tested for PNS Abs with an autoimmune etiology (n = 51), Guillain-Barré syndrome (n = 20, 39%) was the most common diagnosis, with three patients presenting with an acute motor-sensory axonal neuropathy variant (AMSAN), while the others presented with the classic acute inflammatory demyelinating polyneuropathy form (AIDP). Three patients with GBS had a previous history of cancer. Chronic inflammatory demyelinating polyneuropathy (CIDP) was the second most common diagnosis in this group (n = 9, 18%), whereas the remainder of patients (n = 22, 43%) presented with peripheral nervous system involvement in rheumatic or systemic autoimmune disorders.
Toxic and metabolic disorders (n = 40) were the following most common etiologies, including mixed forms (n = 13, 32%), diabetic (n = 7, 17%), chemotherapy-induced (n = 7, 17%), alcohol-related neuropathy (n = 3, 7%), and drug-induced neuromyopathy (n = 3, 7%), followed by other less frequent disorders (n = 7, 17%).
Vascular etiology (n = 11) consisted exclusively of vasculitic involvement of the peripheral nervous system.
Alternative diagnoses with extra-nervous system involvementDiseases without nervous system involvement were identified in 49/661 patients (7%). Vertigo of peripheral origin was the most common etiology in this group (n = 10, 20%), and one of the reasons for Ab testing in few patients was the presence of a concomitant tumor (n = 4). Patients with established extra-NS neoplastic diseases who experienced general medical complications were the second most frequent category (n = 4, 8%). The third group was represented by infections not involving the nervous system (n = 3, 6%). Finally, one last group (n = 32) comprised patients presenting with heterogeneous clinical pictures (e.g., profound asthenia). These presentations could not be framed in a unifying clinical entity and therefore were considered together in this miscellaneous subgroup.
Associations with cancerOverall, 141 tumors were found among the 661 patients with alternative diagnoses considered in the present study (21%). In the CNS disorder group, an associated tumor was identified in 80 patients (20%), including in order of frequency breast (n = 24), hematological (n = 10), lung (n = 9), urinary tract (n = 9), and gastrointestinal (n = 7), followed by other less represented tumors (n = 21). In PerNS disorders, an associated tumor was identified in 45 patients (21%), including in order of frequency breast (n = 16), lung (n = 9), hematological (n = 7), gastrointestinal (n = 5), and others (n = 8). Finally, an associated neoplastic disease was found in 16 patients (32%) with extra-NS involvement, including in order of frequency breast cancer (n = 6), gastrointestinal (n = 3), lung (n = 2), urinary system (n = 2), and hematological (n = 2), followed by one other non-identified primary tumor. Overall, tumors were mostly diagnosed before the neurological syndrome, regardless of the neurological dysfunction location (CNS n = 55 [69%], PerNS n = 30 [67%], and Extra-NS n = 10 [62%]).
A clinical vignette illustrating a neurological syndrome in a patient with breast cancer that was ultimately attributed to an alternative diagnosis rather than PNS is presented in the Supplementary Information.
Laboratory testing yieldConsidering the definite diagnoses of PNS (detailed in [6]), yearly point estimates of diagnostic yield for Ab testing (definite PNS/total number of patients tested) showed a bimodal pattern, but no significant linear temporal variations were evident (p = 0.9 for trend). The yearly number of patients tested increased from 67 (2009) to 131 (2017), a 96% increase. However, diagnostic yield remained low (7% [CI 95% 2–16] vs. 8% [CI 95% 4–14], respectively), while cumulative diagnostic yield was 10% [CI 95% 8–12] during the study period. Among the 661 patients in which an alternative diagnosis was established, only 63 (10%) and 172 (26%) had an initial presentation suggestive of a high-risk or intermediate-risk PNS phenotype respectively, while 426 (64%) did not have a clinical presentation compatible with PNS according to the updated diagnostic criteria [2].
Variable selection and score buildingResults of the logistic regression model are shown in Table 1. Intermediate-risk syndromes or other neurological presentations (OR 7.97, CI95% 3.07–23.80 and OR 192.82 CI95% 66.11–739.59, respectively) and low-risk tumor/absence of tumor (OR 6.90, CI95% 2.75–18.92) were associated with higher odds of an alternative diagnosis than PNS, whereas increasing age (OR 0.95, CI95% 0.92–0.97) was inversely associated with an alternative diagnosis. A distribution of these variables according to the presence of an underlying etiological diagnosis is reported in Table S1. No separation was found among categorical variables in the score model, and therefore, no regularization method was used. However, we note that the size of some of the categorical variables was small as reported in Table S2. Calibration curves alongside Brier scores for the model in the discovery and validation cohorts are presented in Fig. S1. The PNS DDx Score was then derived and pooled into three categories identifying low (− 3 to 0), medium (1–3), and high (> 3) probability of an alternative diagnosis (Table 2). These cut-offs were chosen to maximize specificity.
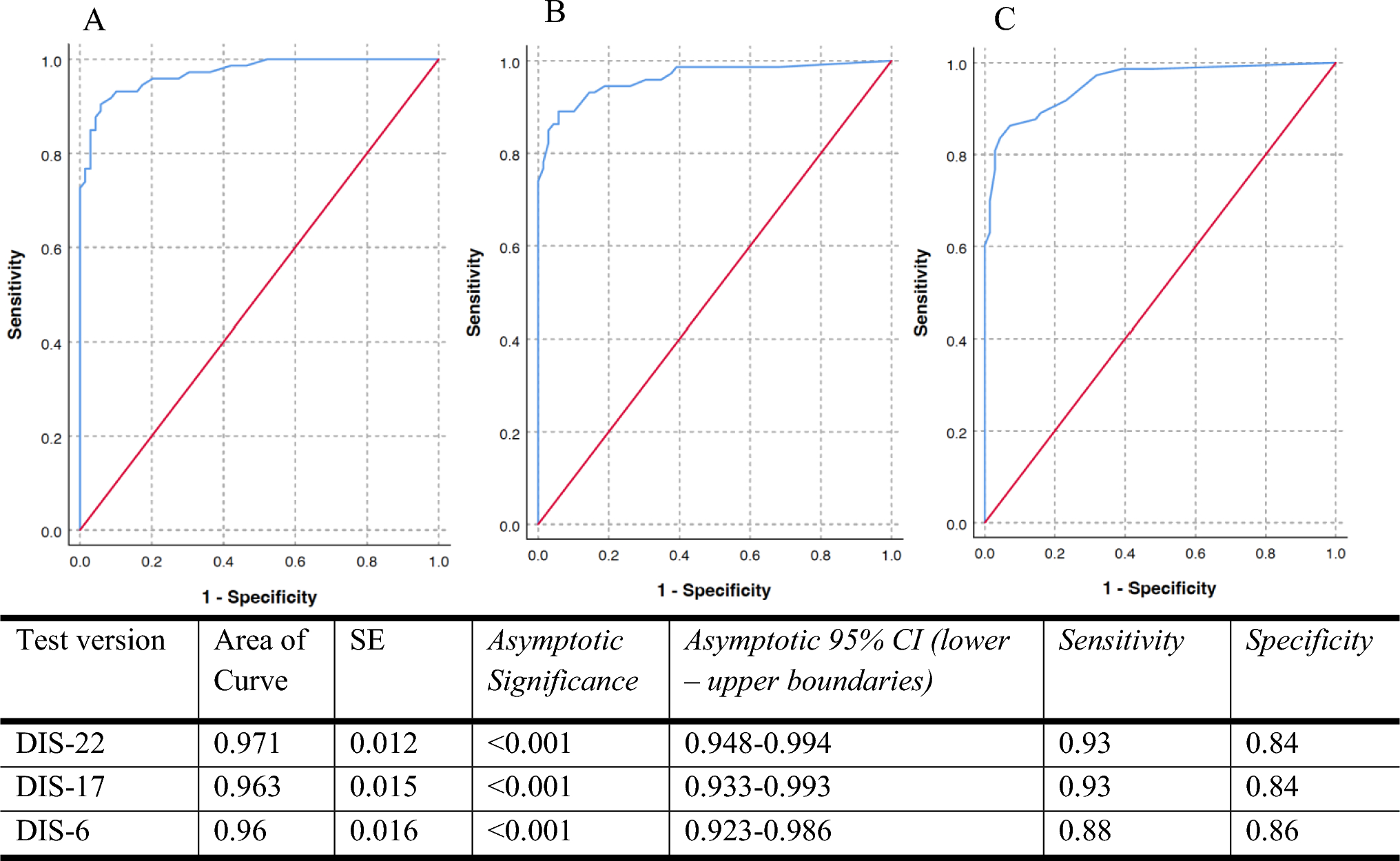
Table 1 Logistic regression model evaluating OR (CI 95%) of an alternative diagnosis of PNSTable 2 PNS DDx Score items, range and point categories for low, medium, and high probability of an alternative diagnosis of PNS, respectively PNS Score validationMean diagnostic accuracy in the derivation cohort was overall good (AUC 0.891, CI95% 0.883–0.971), while the validation cohort outperformed the training set (AUC 0.931, CI95% 0.929–0.997). However, this score was not validated in the possible/probable PNS diagnosis subgroup, as no definite outcome is available for this category. Additional performance metrics are reported in Table S3.
Comments (0)