In Multiple Sclerosis (MS), the identification of easily accessible biomarkers remains a key objective in ongoing research. While Magnetic Resonance Imaging (MRI) has been considered as the laboratory gold standard for detecting disease activity, either through contrast-enhancing lesions or new/enlarging T2-weighted lesions, serum neurofilament light chain (sNfL) has emerged as a promising biomarker reflecting neuroaxonal damage and potentially serving as a prognostic biomarker of disease progression [1, 2].
There is substantial evidence supporting the association between sNfL levels, disease activity, and their prognostic significance [3]. More specifically, high sNfL levels have been associated with future clinical activity, MRI activity, Expanded Disability Status Scale (EDSS) worsening and brain atrophy [4,5,6,7]. Nevertheless, the role of sNfL in the pathogenetic mechanism of MS and its integration as a biomarker in routine clinical practice, remains to be fully elucidated and further investigation is required in order to establish the utility and positioning of sNfL as a biomarker in the evidence based monitoring and management of the disease.
In view of the former considerations, we conducted an observational prospective cohort study, aiming to evaluate the value of baseline sNfL levels, in predicting the achievement of No Evidence of Disease Activity 3 (NEDA-3) status by measuring sNfL during the first clinical evaluation in our MS outpatient clinic; baseline sNfL levels were measured either at the time of diagnosis or during the disease course.
Materials and methods
We prospectively evaluated real world data of MS patients with available sNfL measurements at first clinical evaluation, during a two-year period (June 2023– Apr 2025) in our Outpatient Service (Second Department of Neurology, National and Kapodistrian University of Athens, “Attikon” University Hospital). This study was conducted in accordance with the Declaration of Helsinki principles. Institutional review board approval was obtained from the Ethics Committee of “Attikon” University Hospital (decision number: ΕΒD 318/29- 04–2024). The study was also performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational research [8]. All participants or their legal representatives provided signed informed consent.
The inclusion criteria were (a) age ≥ 18 years old, (b) diagnosis of MS according to the McDonald Criteria 2017, (c) availability of sNfL measurements at baseline evaluation, and (d) availability of imaging data including brain, cervical and thoracic spinal cord MRI, annually or close to a clinical relapse. Patients were evaluated prospectively using the EDSS and NEDA-3 assessment every 6 months or sooner in case of a relapse [9, 10]. MRI and EDSS assessments were performed according to a predefined follow-up schedule, aligned with routine clinical practice. When minor deviations occurred, the closest available assessment was used. Participants with incomplete baseline or follow-up assessments, or who did not consent, were excluded.
The following data were collected for each patient: age, sex, disease duration from onset to baseline sNfL measurement, treatment, Expanded Disability Status Scale (EDSS) and clinical and/or Magnetic Resonance Imaging (MRI) activity, a single baseline sNfL measurement at first clinical evaluation, months until last follow-up assessment, No Evidence of Disease Activity-3 (NEDA-3) and EDSS assessment, and radiological findings during last follow-up. Every follow-up assessment included clinical and MRI evaluation.
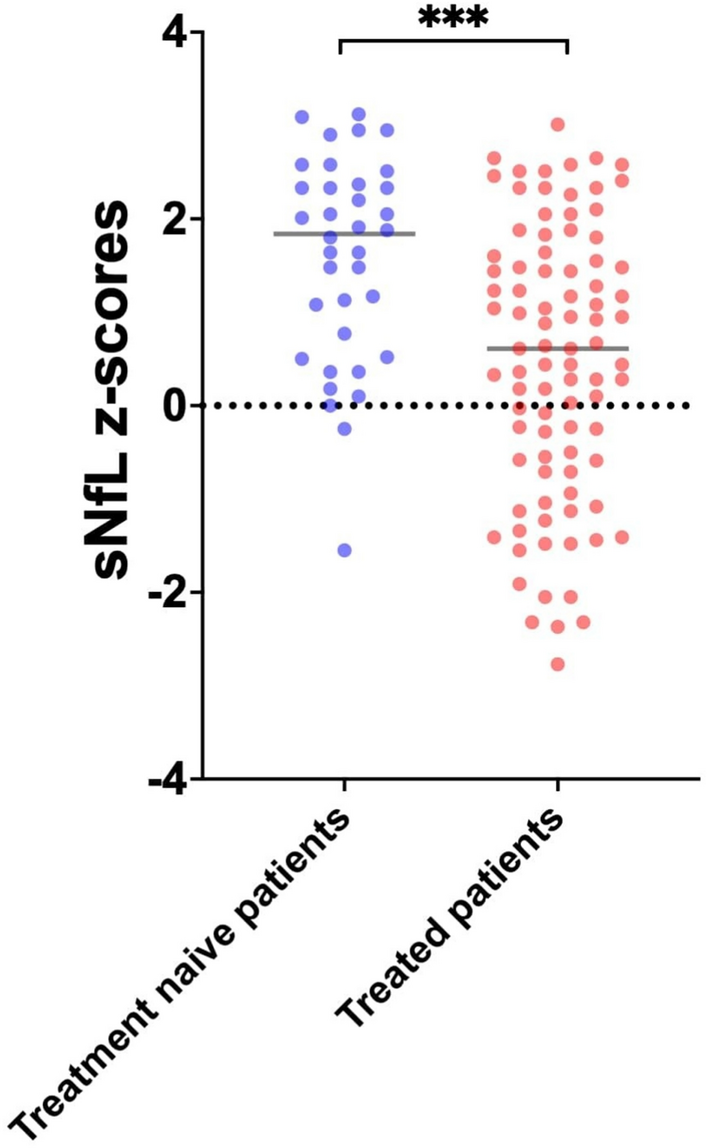
Measurements of sNfL levels were performed during the intial clinical evaluation in our outpatient service (Second Department of Neurology, National and Kapodistrian University of Athens, “Attikon” University Hospital). A peripheral blood sample was drawn from each patient during the baseline clinical evaluation. Single-molecule-array (SIMOA) assay was used for the measurement of sNfL levels. The Nf-Light Advantage PLUS kit of Quanterix was used. sNfL Z‑scores, adjusted for age and BMI, represent a validated prognostic biomarker in MS. High sNfL Z-scores were defined as values above 1.5, whereas values less or equal to 1.5 were defined as low [11, 12]. The threshold > 1.5 is supported by large cohort evidence as indicating higher risk for future clinical or MRI disease activity. The sNfL Z-score > 1.5 was associated with greater risk of future clinical or MRI activity (OR: 3.15; 95% CI, 2.35—4.23; P < 0.0001); this was also the case in patients in NEDA status (OR: 2.66; 95% CI, 1.08—6.55; P = 0.034) [6, 12, 13].
All brain, cervical and thoracic spinal cord MRI results were evaluated by two independent investigators (E-M.D and D.T.) who were blinded to clinical characteristics. All patients underwent either a 1.5 Tesla Tesla (Philips Healthcare, Best, The Netherlands) or a 3 Tesla MRI scan Siemens Magnetom Prisma, Siemens Healthineers, Erlangen, Germany) and continued to be scanned in the same MRI magnetic field strength on follow-up. A comprehensive brain, cervical and thoracic spinal cord MRI protocol with multiplanar reconstruction was used in all participants, which included the following sequences: the T2-weighted sequence, the 3D fluid-attenuated inversion recovery (FLAIR) sequence, the diffusion-weighted imaging (DWI) sequence, the susceptibility-weighted imaging (SWI) sequence and the post-contrast T1-weighted sequence for the brain MRI, as well as T1-weighted, T2-weighted, short tau inversion recovery (STIR), and post-contrast T1-weighted sequences for the spinal cord MRI.
Clinical activity at baseline was defined as clinical relapse occurring within 30 days prior to the baseline evaluation and MRI activity was defined as gadolinium-enhancing lesions or new or enlarging T2 lesions within 30 days prior to the baseline evaluation.
Achievement of NEDA-3 during follow-up was predefined as the main outcome of our study. EDSS was used as a clinician-administered assessment scale of worldwide acceptance in order to evaluate the functional systems of the central nervous system [9] Moreover, NEDA-3, defined as a composite of three related measures, namely no clinical relapses, no sustained disability progression (as defined by no increase in the EDSS-score), and no activity seen on MRI (new or enlarging T2 hyperintense lesions or gadolinium-enhancing lesions) during a specified time period was used [10]. Achieving NEDA-3 during the last follow-up was defined as the main outcome.
Statistical analysis
Categorical variables are presented as mean ± standard deviations (SD) for continuous variables with normal distribution or as median with interquartile ranges (IQRs) in cases of skewed distributions. Comparisons of different variables were expressed using the unpaired t-test or the Mann–Whitney U test. Statistical significance was defined as a p-value < 0.05.
Single and multivariable linear regression models were performed to identify predictors of baseline sNfL Z-score. Univariable and multivariable Cox proportional hazards regression models were used to evaluate the association of sNfL with NEDA-3 during last follow-up. The model included baseline sNfL levels (high vs. low), EDSS score at the time of baseline sNfL measurement, MS subtype at baseline (relapsing–remitting MS vs. progressive MS), and the presence of gadolinium-enhancing (Gd +) lesions at baseline. Covariates were selected a priori based on clinical relevance and prior literature, and no automated variable selection procedures were applied. The proportional hazard assumption was assessed using Schoenfeld residuals and log–log survival plots. All analyses were performed using the R–software version 2025.05.0 + 496 and GraphPad Prism-10.

Comments (0)