
Remember me
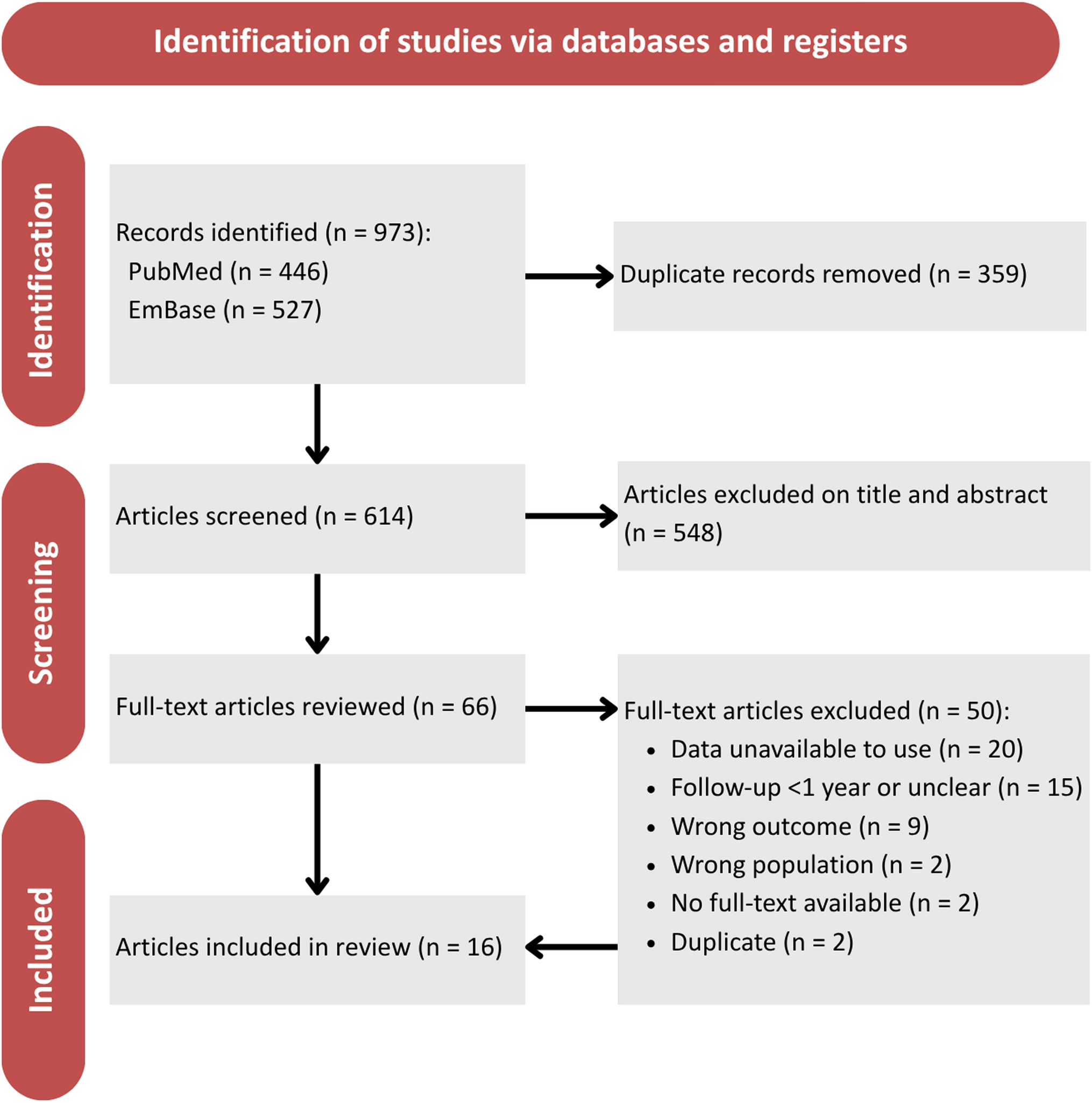
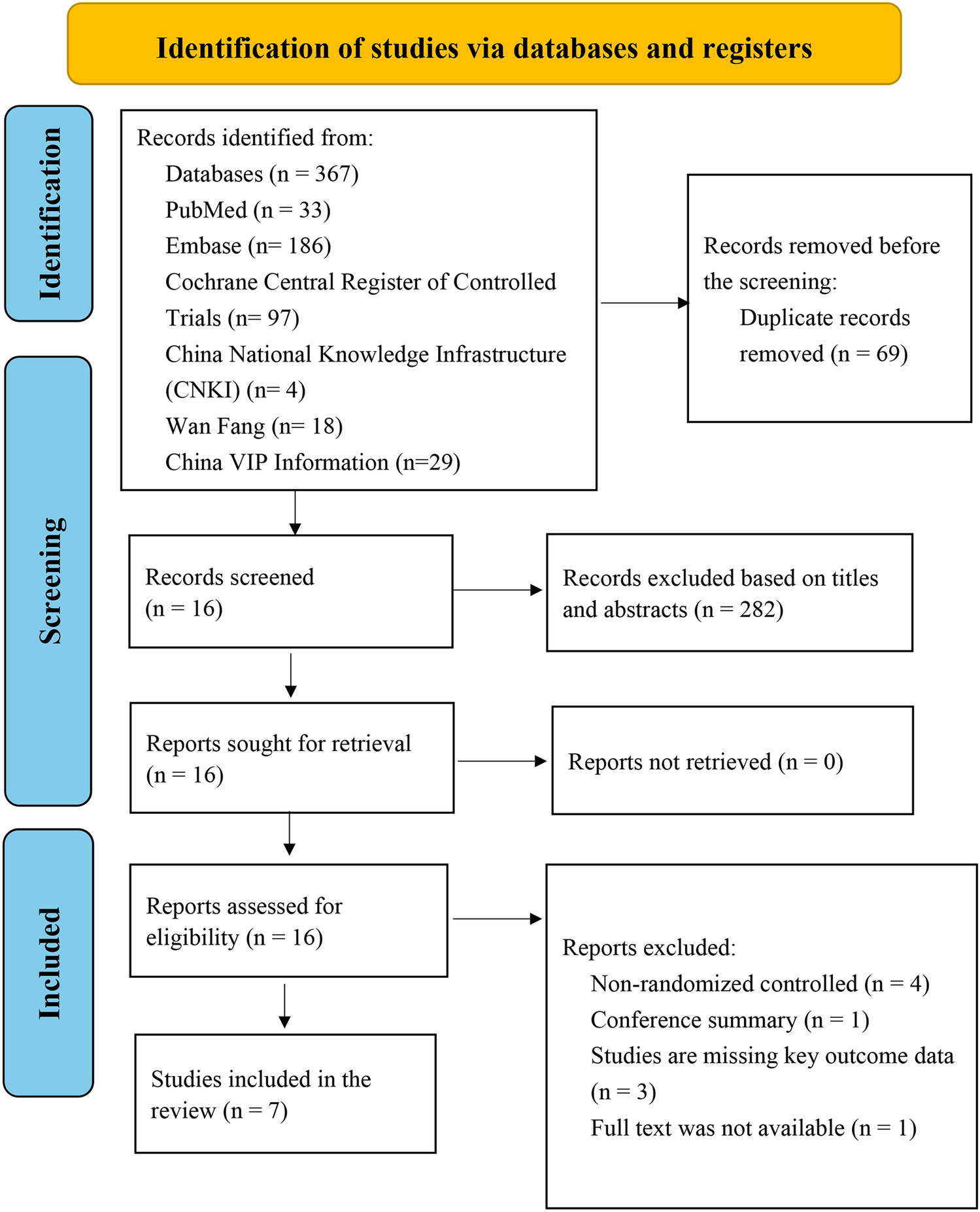
A comprehensive electronic literature search was conducted across PubMed, Cochrane, Web of Science, and Scopus databases, yielding a total of 7,326 records. After removing 2,032 duplicate entries and 37 entries identified by automation tools, 4,923 distinct studies were available for title and abstract screening. Initial screening of titles and abstracts resulted in the exclusion of 4,699 studies, leaving 224 articles for full-text assessment. Ultimately, 13 studies met all eligibility criteria and were included in this systematic review and meta-analysis. The detailed screening process is illustrated in the PRISMA flow diagram (Fig. 1).
Fig. 1
PRISMA flow diagram of the selection process
Study characteristicsThe selection process resulted in 13 eligible studies comprising a total sample size of 6,198 patients [12,13,14, 16,17,18,19,20,21,22,23,24,25]. These included nine retrospective cohort studies, three prospective observational studies, and one post-hoc analysis of a randomized controlled trial (RCT). Studies were published between 2016 and 2025 and included adult patients undergoing mechanical thrombectomy (MT) for acute ischemic stroke. All included studies were multicentric, conducted across various regions, including Europe (Germany, Netherlands, Sweden, France, Austria), North America (USA, Canada), and Asia (Korea, China). The interventions primarily involved thrombectomy with or without intravenous thrombolysis. Detailed characteristics and baseline data of included studies are summarized in Tables 1 and 2.
Table 1 Summary of the included studiesTable 2 Baseline characteristics of the included studiesQuality assessmentThe risk of bias assessment was conducted using the Newcastle–Ottawa Scale (NOS), evaluating selection, comparability, and outcome domains. Most included studies demonstrated high methodological quality, scoring between 7 and 9 out of a possible 9 points. Specifically, six studies scored 9 points, indicating very high quality, while seven studies scored 8 points, indicating good quality. A detailed illustration of the risk of bias assessment is presented in Table 3.
Table 3 Risk-of-bias assessment results using the Newcastle–Ottawa Scale (NOS)Clinical outcomes90-day favorable outcome (mRS 0–2)Seven studies assessed the impact of thrombus migration on favorable neurological outcomes at 90 days, defined as modified Rankin Scale (mRS) scores between 0 and 2. Meta-analysis demonstrated that thrombus migration was significantly associated with improved favorable outcomes compared to the non-migration group (OR = 1.43, 95% CI [1.05–1.95], P = 0.025). However, significant heterogeneity was observed (I2 = 71%; P = 0.002) (Fig. 2A).
Fig. 2
Forest plots of functional outcomes. (A) 90-Day favorable outcome (mRS 0–2), (B) successful reperfusion (TICI 2b-3), (C) NIHSS change from baseline to discharge
Successful reperfusion (TICI 2b-3)Meta-analysis of ten studies revealed no statistically significant difference in successful reperfusion rates (TICI 2b-3) between thrombus migration and non-migration groups (OR = 0.69, 95% CI [0.46–1.03], P = 0.07). Significant heterogeneity was identified (I2 = 73.7%; P < 0.0001) (Fig. 2B).
NIHSS change from baseline to dischargeFive studies assessed changes in NIHSS scores from baseline to discharge. There was no significant difference in neurological improvement between the thrombus migration and non-migration groups (MD = 0.36, 95% CI [-0.17–0.90], P = 0.18). No heterogeneity was detected (I2 = 0%; P = 0.69) (Fig. 2C).
90-day mortalityAnalysis of five studies evaluating the impact of thrombus migration on 90-day mortality revealed no significant difference between thrombus migration and non-migration groups (OR = 0.86, 95% CI [0.69–1.06], P = 0.15). There was no heterogeneity among these studies (I2 = 0%; P = 0.83) (Fig. 3A).
Fig. 3
Forest plot of safety outcomes. (A) 90-Day mortality, (B) symptomatic intracranial haemorrhage (sICH), (C) any intracranial hemorrhage (ICH)
Symptomatic intracranial haemorrhage (sICH)Five studies evaluated the incidence of symptomatic intracranial haemorrhage. No significant difference between groups was observed (OR = 1.12, 95% CI [0.78–1.61], P = 0.54), with no heterogeneity (I2 = 0%; P = 0.92) (Fig. 3B).
Any intracranial haemorrhage (ICH)Data from four studies indicated a statistically insignificant difference in ICH between the two groups (OR = 1.25, 95% CI [0.47–2.10], P = 0.48). moderate heterogeneity was observed (I2 = 54%; P = 0.1013) (Fig. 3C).
Leave one out sensitivity analysisWe conducted sensitivity analyses to assess the single study effect on the robustness of the results (Supplementary file 2). For symptomatic ICH and mortality, odds ratios (ORs) remained close to 1.0 with low heterogeneity (I2 = 0%), suggesting consistent findings across studies. In contrast, favorable outcomes at 90 days showed more variability (I2 up to 76%), with statistical significance sensitive to certain study removals. 90 days Mortality and Mean change in NIHSS showed similar effect size upon removing any of the studies with homogenous results (I2 = 0). Successful reperfusion outcomes demonstrated moderate-to-high heterogeneity (I2 ≈ 70–77%), though effect sizes were relatively stable. Overall, the analysis suggests that no single study disproportionately influenced the meta-analysis conclusions, though some endpoints—particularly functional recovery and reperfusion—show notable heterogeneity that may reflect differences in patient populations or treatment protocols.
Comments (0)