Considering the importance of the purinergic system and oxidative stress in modulating platelet activity and the fact that physical exercise is capable of modifying its parameters in a useful way, this study investigated the effects of mixed circuit physical training on the activity of ectonucleotidases in platelets, serum ATP levels, and serum oxidative stress components. Hemodynamic, anthropometric, and biochemical parameters (concerning the glycemic and lipid profile) were also considered.
Although the present study provides important insights into how type 2 diabetes modulates the platelet and redox responses to mixed circuit training, we recognize a methodological limitation regarding the absence of a non-exercising control group. Both the diabetic and normoglycemic groups underwent the same training protocol; therefore, our findings do not allow conclusions about the isolated efficacy of exercise compared to a sedentary condition. Instead, the study was designed to evaluate differential physiological adaptations to exercise between distinct glycemic profiles. All participants were sedentary at baseline, and pre-intervention measurements served as internal controls, minimizing interpersonal variability and preventing the introduction of additional confounding factors that would arise from separate non-exercising groups. This approach is frequently adopted in exercise physiology research and is appropriate for investigating relative changes induced by training within the same individuals. Nevertheless, we acknowledge that the absence of a non-exercising group limits causal inference regarding exercise per se, and this should be taken into account when interpreting the results. Future studies should incorporate an additional sedentary control arm to determine the absolute contribution of exercise to the observed effects.
Regarding hemodynamic parameters, it is already established in the literature that T2DM decompensation modifies blood pressure levels [37], increasing the risk of cardiovascular events. The results of this study are in agreement with the already known [38,39,40,41] impacts of physical exercise on hemodynamic aspects found in the literature. SBP analysis showed a significant decrease after the mixed circuit exercise protocol, especially in the diabetes group. In contrast, DBP did not change significantly after 16 weeks of training.
Meanwhile, it is expected that individuals without T2DM will present an HbA1c < 6, which is in line with what was observed in our control group both pre- and post-intervention. HbA1c reflects the body’s glycemic levels in the last 3 months, being an important tool for assessing blood glucose levels in T2DM [42]. In the pre-intervention period of our study, HbA1c had increased values in the DG compared to the CG, which was already expected and reinforced that participants from the control group did not have T2DM.
About the lipid profile, it is known that elevated LDL and TG levels increase the risk of cardiovascular disease [43], at the same time that T2DM also expands the risk of these events [44]. This reinforces the importance of following the therapeutic goals of TC, HDL, LDL, and TG levels recommended by the American Diabetes Association (ADA) [45].
In our study, a tendency to increase TC levels in the DG was observed, which may be associated with an expansion in HDL that is useful for removing excess LDL deposited in the blood vessels. This improvement can be strongly associated with physical exercise, considering that the volunteers did not make dietary interventions, which were evaluated through questionnaires about eating habits applied before and after physical training. Concerning TG values, there was no change with statistical significance after the physical training protocol. In this case, dietary modifications associated with physical exercise are strongly recommended to reduce TG rates [43].
Related to the anthropometric results, no significant reductions were observed in body weight, BMI, WC, CCO, TAV, MM, and MA after 16 weeks of mixed circuit physical training. Although a percentage tendency in decreasing TAV can be observed in both groups, this is an important result considering the contribution of adipose tissue to systemic insulin resistance, especially through the production of free fatty acids [46]. Studies that carried out intervention for a longer period [47] or with a greater frequency of physical exercise [48, 49] showed significant improvement in the anthropometric variables analyzed.
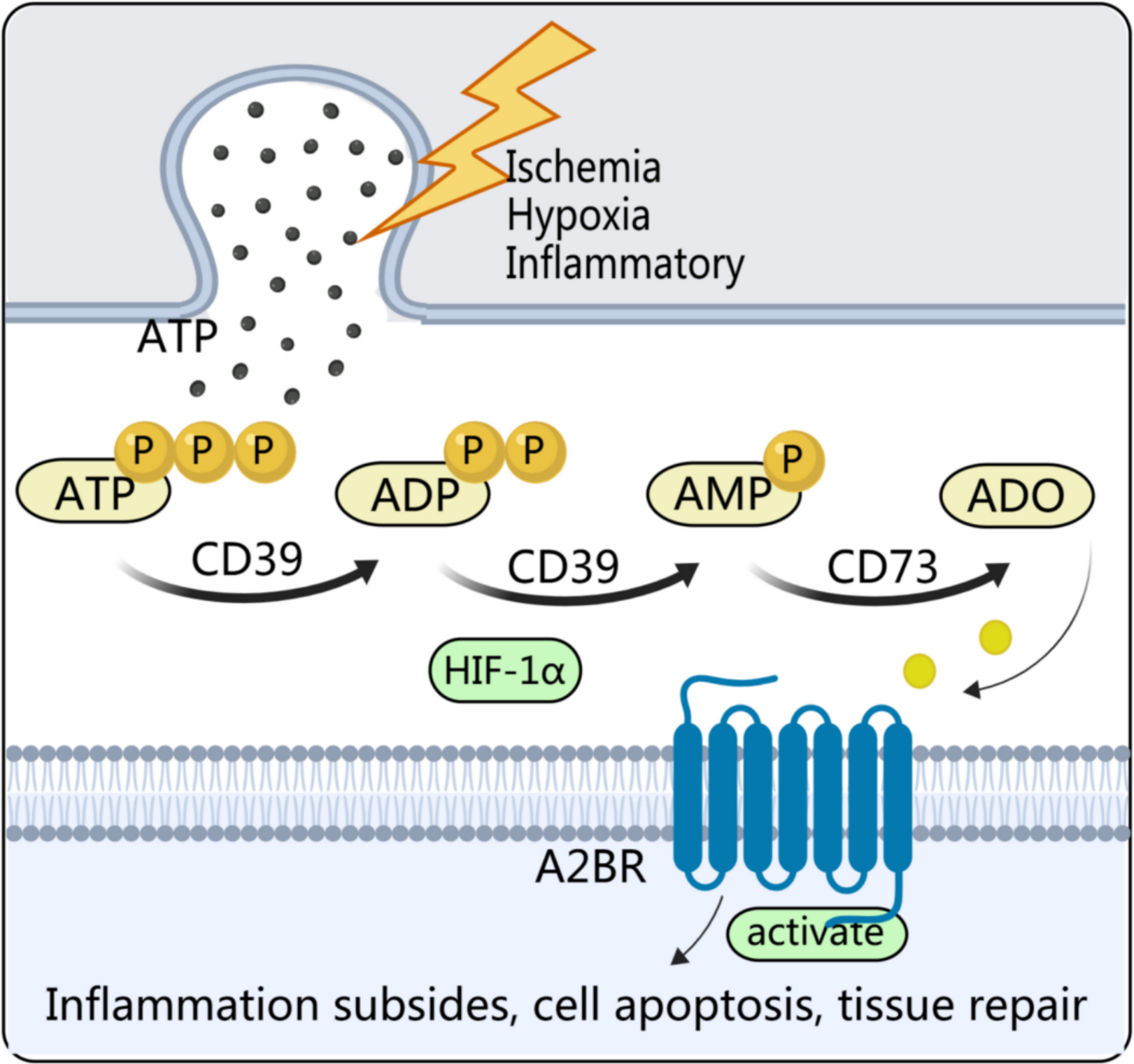
Regarding the parameters of the purinergic system evaluated in platelets, it has been proved that nucleotides and nucleosides play an important role in thrombotic regulation. ADP is one of the main promoters of platelet aggregation, activating platelets and causing them to adhere to the initial layer, expanding the thrombus [50]; this role is already well established and important antiplatelet agents act in this process, inhibiting P2Y receptors on platelets [51]. Adenosine is an inhibitor of this process through A2 receptors, increasing the intracellular concentration of cyclic AMP (cAMP) and, as a result, inhibiting platelet activation [52]. Within this context, the enzymes NTPDase and NT5 perform an important role in regulating platelet activity by modulating the presence of ADP and adenosine in the extracellular environment.
The literature shows that people with T2DM have increased E-NTPDase and E-NT5 activity, probably as a compensatory mechanism for the increase in nucleotides in the extracellular environment [53]. Physical exercise directly affects purinergic signaling and consequently, the activity of enzymes that hydrolyze nucleotides. Moreover, it has been observed that, acutely, exercise increases the capacity of these enzymes, which hydrolyze ATP, ADP, and AMP into adenosine [20, 54].
Findings from Martins et al. [55] demonstrated that the usual modifications from metabolic syndrome that precedes T2DM were reversed with regular physical activity, showing a decrease in the activity of E-NTPDase and E-NT5; also, a decline in coagulability modifications related to exercise. It is also important to highlight that the reduction in E-NTPDase activity might involve distinct regulatory mechanisms beyond direct downregulation. It is possible that MCT reduced platelet activation and turnover, leading to lower expression of the enzyme on the platelet surface. Although molecular expression of purinergic enzymes was not evaluated here, future studies should include protein expression analyses to clarify the regulatory pathways involved.
Furthermore, the thrombus microenvironment is composed of other cells such as the ones from the immune system and, mainly, endothelial cells, which also play a regulatory role in platelet activity. In this sense, it was demonstrated the importance of ectonucleotidases in endothelial cells to inhibit platelet activation and aggregation [56], making it necessary, in the future, to study how mixed circuit training affects these cells.
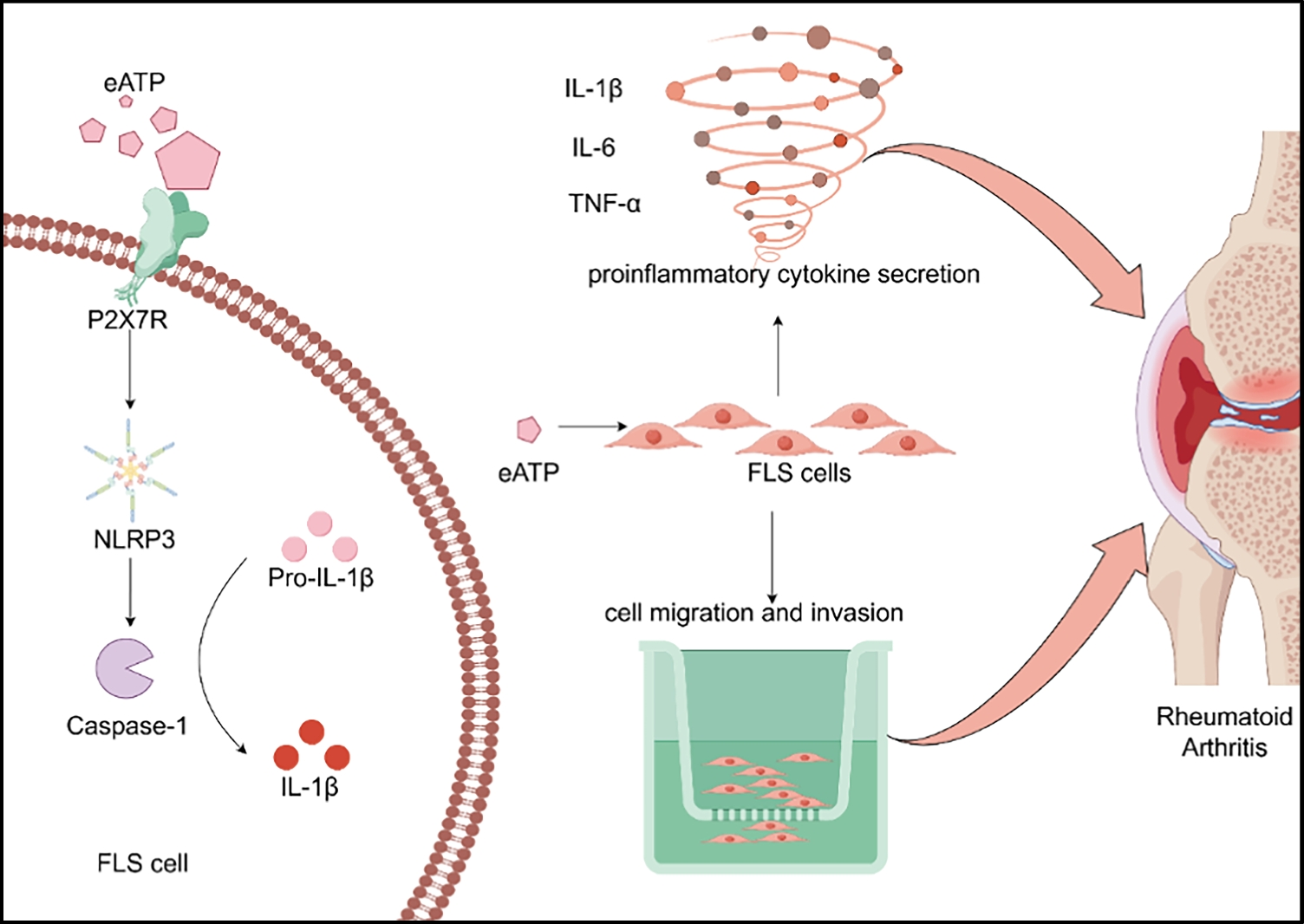
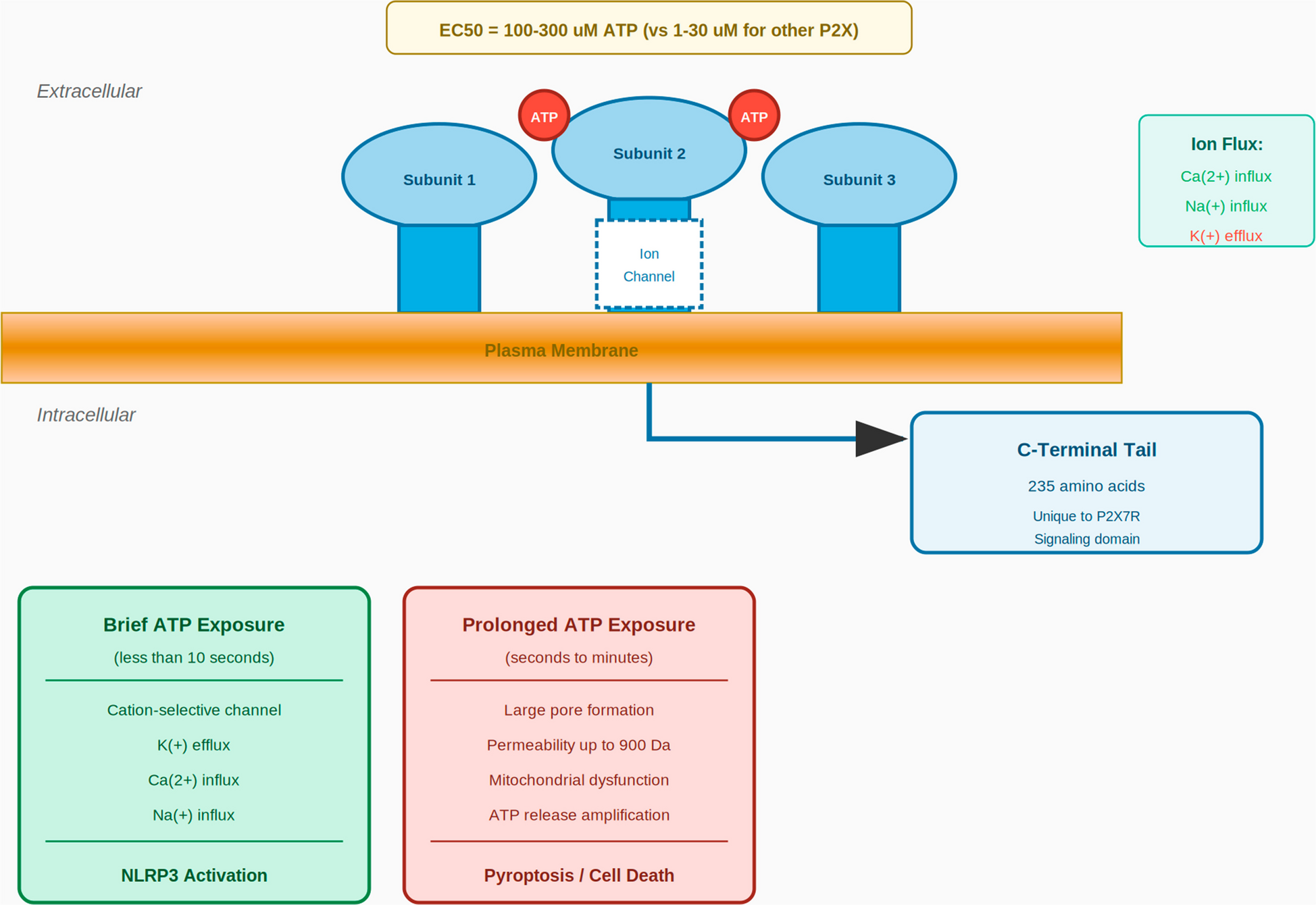
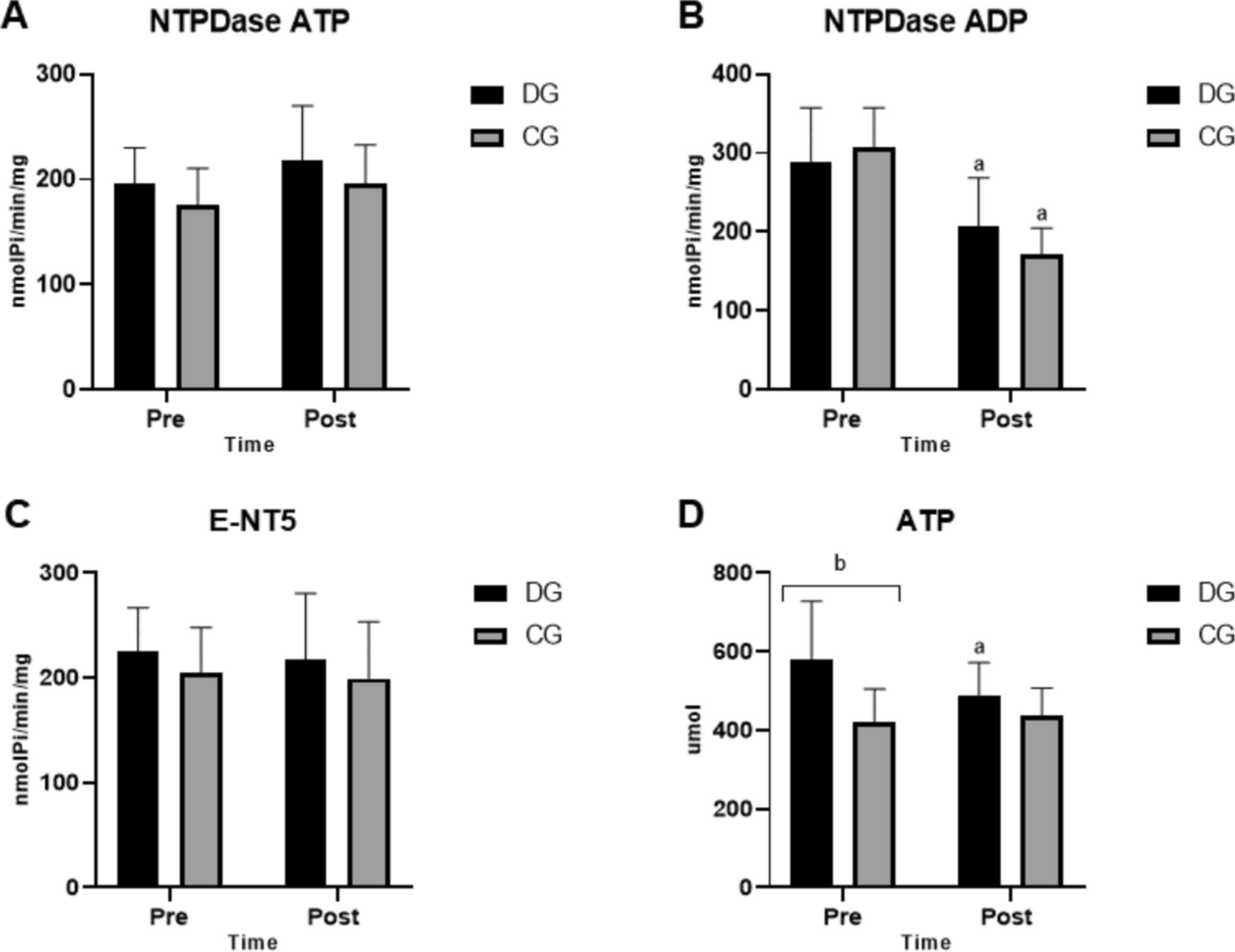
Still on the purinergic signaling, about serum ATP levels, the concentration of this nucleotide significantly increased in the diabetes group compared to the control before the intervention was performed, reinforcing that diabetes promotes an increase in ATP, activating more P2X type receptors [57]. These receptors are capable of regulating platelet activation, both directly, via P2X1 (promoting platelet activation) and P2X7 (inhibiting platelet activation), and indirectly by activating immune system cells that promote platelet activation [58].
In this study, no change in the activity of ectonucleotidases was observed between groups before the intervention protocol. However, after the mixed circuit training exercise, a decrease in E-NTPDase activity for the hydrolysis of ADP was observed, as supported in the literature. Yet, the activity of E-NTPDase for the hydrolysis of ATP and E-NT5 did not change.
It is important to highlight that both ATP and ADP exert pro-aggregatory effects on platelets, although through distinct purinergic receptors. ATP activates P2X1 receptors, inducing rapid calcium influx and platelet shape change, while ADP acts primarily via P2Y receptors to sustain aggregation. Therefore, reductions in extracellular ATP levels—such as those observed after MCT in the diabetic group—may attenuate upstream substrate availability for ADP generation and diminish ATP-mediated platelet activation pathways. This mechanistic interplay helps explain how a decrease in E-NTPDase activity for ADP hydrolysis can coexist with a reduction in ATP concentration without indicating a pro-thrombotic shift.
Moreover, enzymatic activity within the purinergic pathway typically responds to fluctuations in substrate concentration, a phenomenon consistently demonstrated in experimental studies. Thus, the observed reduction in E-NTPDase activity may reflect a physiological adaptation to lower extracellular ATP availability, rather than a mechanism favoring platelet aggregation. Taken together, these findings suggest that MCT induces a coordinated modulation of purinergic signaling elements, favoring reduced nucleotide-driven platelet activation despite decreased ADP hydrolysis.
On the other hand, after mixed circuit training, there was a significant decrease in ATP concentration in the diabetes group, demonstrating that exercise is an important regulator of the purinergic system, considering that a decrease in ATP concentration results in lower activity of P2X receptors that exacerbate platelet activity [58]. Furthermore, the decrease in the extracellular concentration of ATP associated with a decrease in the activity of enzymes demonstrates a balance of the components of the purinergic system, characterized by a change in the pattern of this signaling as a whole.
Although E-NTPDase activity decreased after MCT, extracellular ATP levels were also reduced, which may appear contradictory at first. However, extracellular ATP is determined not only by its degradation but primarily by its release [53]. MCT likely reduced ATP release by lowering basal platelet activation and decreasing inflammatory and oxidative stimuli that trigger ATP efflux. Therefore, even with a reduction in E-NTPDase activity, the net extracellular ATP concentration decreased due to lower cellular release. This suggests that MCT decreases pro-thrombotic signaling independently of enzymatic degradation.
In addition, the association of the purinergic system with oxidative stress seems to play an important role in the prothrombotic state of T2DM. Lipid peroxidation of the phospholipid membrane [59], characteristic of states with high oxidative stress, causes dysfunction of the NTPDase enzyme, reducing its activity [60].
Regarding the oxidative stress parameters evaluated, thiols are non-enzymatic antioxidants that help in the structural protection of cells. In the literature, it was observed that in T2DM, there is a reduction of thiols, and this is correlated with an increase in glycation products, which are markers of advancement and the presence of complications [61]. However, in our results, it was not possible to observe a statistically significant change in this parameter between groups or before and after the intervention.
Another antioxidant evaluated was GST, an enzyme that acts by suppressing the formation of free radicals that accentuate oxidative stress [62]. Studies already demonstrate the increase of GST-dependent antioxidant defenses after resistance and sprint training protocols, so their levels can be associated with physical activity [63, 64]. Furthermore, it has also been demonstrated that GST can play a role in inhibiting platelet aggregation induced by ADP [65]. Similarly, in our study, both groups increased GST activity after the mixed circuit training protocol.
Vitamin C (or ascorbic acid) is an important antioxidant that eliminates ROS [16]. In the literature, it has been demonstrated that, in addition to its antioxidant effect, vitamin C intensifies the formation of prostaglandin E1. This metabolite increases the action of insulin and also plays an antiplatelet action [66], which reinforces the importance of increasing levels of this compound in people with T2DM.
However, when searching for information about the impact of physical exercise on vitamin C, most studies added oral vitamin C supplementation to the training protocols [67,68,69], and studies that demonstrate the effect of physical exercise alone are hard to find, reiterating the importance of the results found in our study. In this context, after 16 weeks of circuit training, the diabetes group showed a significant increase in vitamin C levels, without its exogenous supplementation.
The activity of MPO was evaluated, an oxidizing enzyme that produces reactive species that attack and modify the function of healthy cells [70]. Its activity showed a significant decrease after 16 weeks of mixed circuit training, especially in the diabetes group. Also, it has already been reported in the literature that increased MPO activity is associated with higher glucose and HbA1c levels [71] and that it can interact with and activate platelets [72]. So, like ADP, it acts in favor of platelet aggregation, predisposing pro-thrombotic events, which explains its importance in the context of T2DM.
This study was not randomized, as the allocation to groups was defined by the presence or absence of type 2 diabetes, a pre-existing clinical condition. Although this design allowed for the evaluation of differential physiological responses to the same exercise protocol, it may introduce selection bias and limit causal inference. Therefore, the findings should be interpreted considering this methodological constraint.
Finally, our findings reveal consistent modulation of purinergic and oxidative pathways, although the absence of multivariate approaches limits a more integrated interpretation of these variables. Future studies should incorporate multidimensional analysis to explore whether these changes correlate directly and to provide a deeper understanding of the mechanisms underlying the effects of MCT.

Comments (0)