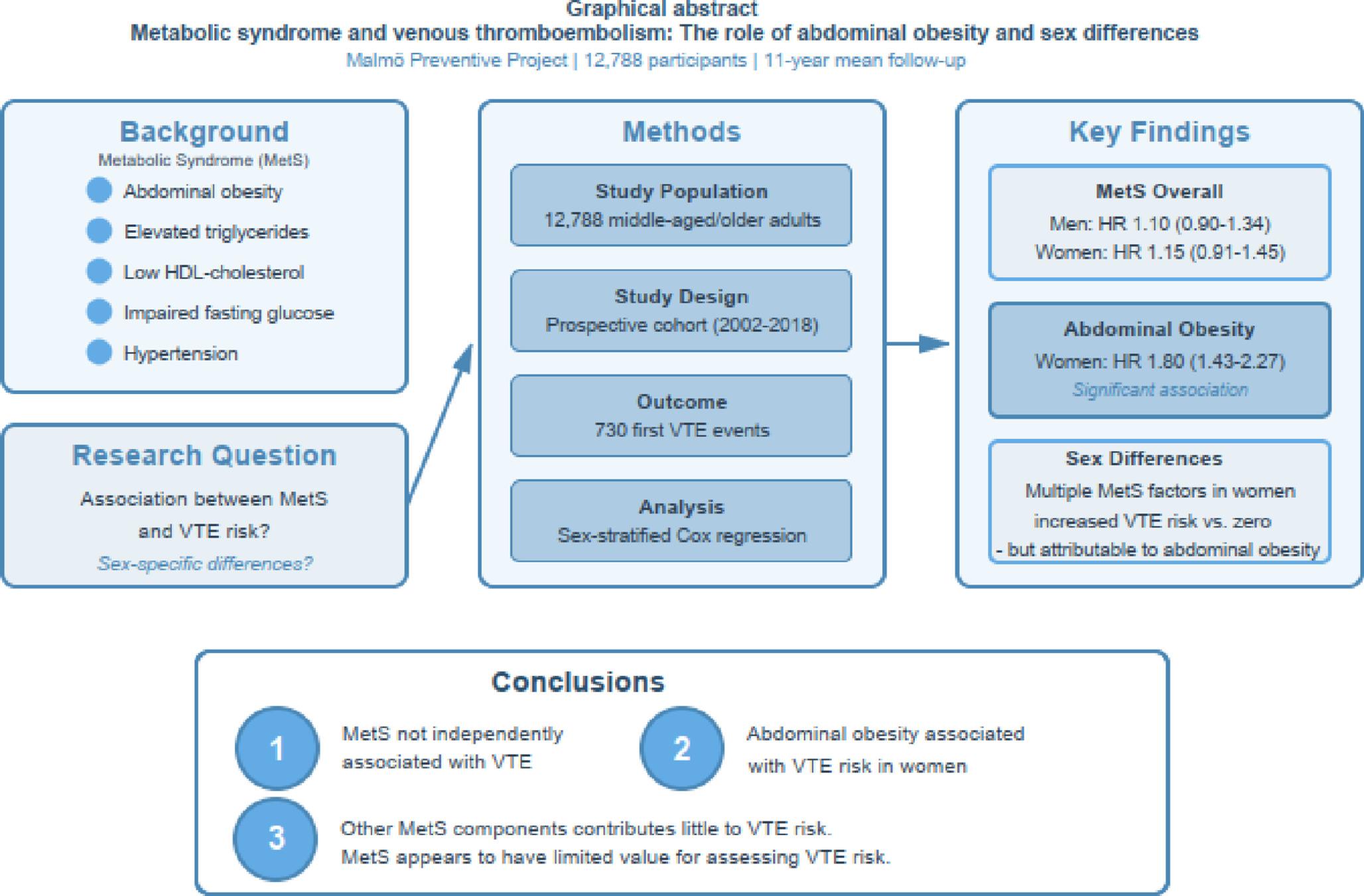
The present cohort study of 12,788 Swedish men and women with a mean follow-up time of 11 years found no association between dichotomously defined MetS and VTE risk, in either sex, both in univariate analyses and after adjusting for potential confounders (age, height, and smoking). Abdominal obesity was associated with VTE risk only in women, as shown in the adjusted analysis (HR 1.80; 95% CI 1.43–2.27). An overall increased risk was observed among individuals with abdominal obesity in stratified analyses, with a more pronounced effect in women. Also, a dose-dependent increased risk of VTE from increased waist circumference was most obvious in women. This suggests that the higher VTE risk seen in women with multiple MetS factors compared to zero is largely attributable to abdominal obesity. Supporting this interpretation, the other MetS factors showed no significant impact on VTE risk in individuals without abdominal obesity. Moreover, there was no discernible trend of an increasing VTE risk with an increasing number of MetS factors, as was found by Borch et al. [16]
Our results differ somewhat from previous research by Steffen et al. [17], who found MetS to be associated with risk of total VTE (provoked and unprovoked) among men only, and Borch et al. [16], who found MetS to be associated with provoked VTE but not unprovoked, in both sexes. Different inclusion/exclusion criteria might explain the divergent findings, which are also seen in our sensitivity analysis, showing slightly altered HRs after including participants with baseline comorbidities. Other demographic profiles and genetic backgrounds may also cause some of the divergent results. Additionally, adjustments in Cox regression models differ between studies. As an example, Park et al. [19] found an association between MetS and VTE risk in a model adjusted for sex, age, smoking, exercise status, family history of hypertension, stroke, heart disease, and diabetes, but after including BMI and cholesterol, among other variables, associations were attenuated. This exemplifies the challenge in comparing these different study results.
Although our adjusted analysis only found women with abdominal obesity to have an increased risk of VTE, men also showed an increased risk in univariate analysis, but associations were attenuated after adjusting for potential confounders. Height has been identified as a risk factor for VTE in both men and women, although results are more consistent for men [39,40,41,42]. Thus, adjusting for height in men may attenuate the association between waist circumference and VTE, as some of the risk attributed to abdominal obesity may actually reflect risk driven by greater body size or stature. Such attenuation was confirmed in a separate analysis of our data (Supplementary Table 2). This supports the idea that abdominal obesity plays a more significant role in VTE risk among women. Other studies have found that abdominal obesity carries a risk in both sexes [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,, 14, 43, 44], including one that also adjusted for height in their models [45]. Similar to our results, Brink et al. [46] found abdominal obesity linked to PE and DVT in women but not in men, in a Swedish cohort using similar exclusion criteria and also adjusting for height. When they included patients with cancer before baseline and cancer-related VTE incidents, the risk was also present in men. Hence, they hypothesize that the association between men with abdominal obesity and the risk of DVT and PE may be mediated through cancer-related pathways. Obesity is a risk factor for cancer, and it promotes carcinogenesis through interlocking of not only metabolic but also inflammatory, immune, and hormonal pathways. Moreover, biological plausibility and convergent epidemiology support obesity as a modifiable cancer risk factor [47]. Given the mixed findings in previous research, it is difficult to conclude whether abdominal obesity independently increases risk in men, or if the observed association is confounded by other factors such as cancer or height. Our results showed that the other individual MetS factors (excluding waist) have little impact on VTE risk, in alignment with previous research stating that traditional cardiovascular risk factors lack an association with risk of VTE [13, 28]. However, we found that IFG and hypertension increase the risk of DVT specifically in women. Borch et al. [16] observed similar associations, but only in univariate analysis and with both sexes combined.
The pathophysiological link between obesity and VTE is multifactorial. Increased intra-abdominal pressure reduces venous return from the lower limbs and slows venous flow, promoting venous stasis [15]. Obesity is also associated with elevated plasminogen activator inhibitor-1, which inhibits fibrinolysis and promotes a prothrombotic state [15, 48]. Additional haemostatic changes include higher circulating levels of fibrinogen and factor VIII [15]. Additionally, the inflammatory activity of adipose tissue, causing increased levels of C-reactive protein, IL-6, and TNF-α, contributes to oxidative stress, which in turn promotes platelet aggregation, endothelial dysfunction, and thrombus formation [15]. These haemostatic, inflammatory, endothelial, and flow-related mechanisms may explain why adiposity appears to be the dominant metabolic factor associated with VTE risk. Some previous research reports stronger associations between circulating levels of fibrinogen and C-reactive protein in women with obesity than in men [49], which may partly explain our finding that abdominal obesity was linked to thrombotic risk predominantly in women. Our results add to the growing body of evidence on obesity’s adverse health effects and underscore the potential clinical benefits of early lifestyle interventions. Clinicians should also remain mindful of potential sex-specific differences that may not be captured by standard risk assessments.
The population-based cohort used in this study offers several strengths, including a large sample size, long-term follow-up, and outcome data derived from national registries. A case validity of 95% has been reported in a study examining VTE in the National Patient Register [31]. The overall positive predictive values of diagnoses in the Swedish Hospital Discharge Register are estimated to be about 85–95% [22]. Sex stratification and separate analyses of PE and DVT outcomes provide a more detailed assessment of the associations.
A limitation of our study is that MetS factors were only collected at baseline (re-examination) and not updated over time. This limits our ability to account for changes in metabolic health during follow-up. However, weight gain over time is more common than weight loss [50]. Another limitation is the lack of information on physical activity and cardiorespiratory fitness. We had no access to detailed information about medication for blood lipids, blood pressure treatment, and drug treatment for elevated glucose, which is a limitation. We had no information about anticoagulant treatment, which is a limitation. However, we excluded patients with VTE or arterial cardiovascular disorders at baseline, i.e. individuals at increased risk of receiving anticoagulation treatment. Different study designs, MetS definitions, and exclusion criteria might make risk estimates difficult to compare across studies. As an example, a meta-analysis by Abuduhalike et al. [51] used BMI instead of waist circumference as obesity measurement, hindering a comparison of results. Although major factors like cancer and CVD were excluded, our study lacked data on recent surgery and immobilization. Thus, our definition of VTE is not strictly “unprovoked” or “idiopathic” as defined by some previous authors [16,17,18], making the findings less generalizable. Finally, the cohort included more men than women, limiting generalizability to a balanced general population.

Comments (0)