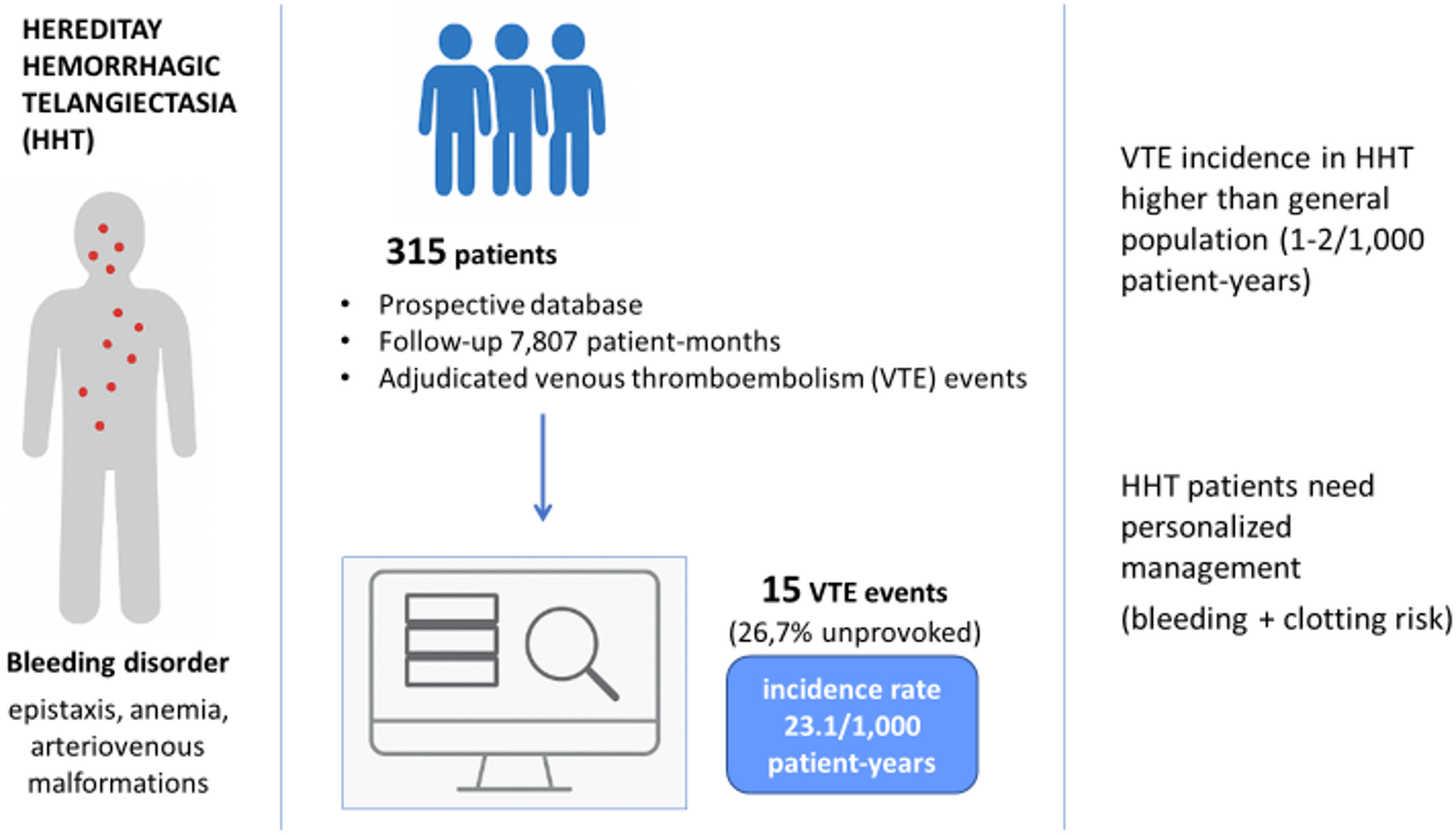
This prospective registry-based study evaluated the incidence of VTE in patients with HHT using adjudicated outcomes. Among more than 300 patients, we observed an incidence rate of 23.1 per 1,000 patient-years, rising to 45.1 per 1,000 patient-years in individuals aged > 65 years. These rates are markedly higher than the 1–2 per 1,000 person-years reported in the general European population [7] and exceed the expected 6–8 per 1,000 person-years for adults aged 65 years and older [8, 9], underscoring that VTE is an underrecognized complication in HHT.
Our results align with previous retrospective studies suggesting increased thrombotic risk [3,4,5], though they contrast with the Danish case–control study that found no excess events [6]. The prospective registry design, systematic event adjudication, and verification with medical records minimize the risk of underreporting and strengthen the validity of our findings.
The mechanisms remain uncertain. Chronic iron deficiency anemia, leading to elevated factor VIII, is the most widely proposed explanation [3,4,5,6], but endothelial dysfunction or systemic inflammation may also contribute. Notably, more than one-quarter of VTE events were unprovoked, supporting the hypothesis of disease-related prothrombotic mechanisms. In our cohort, patients who developed VTE were significantly older and had a higher prevalence of cancer compared with those without VTE, consistent with well-established risk factors that may further amplify thrombotic susceptibility in HHT.
Analysis of provoking factors highlighted missed opportunities for prophylaxis. None of the four patients who developed VTE during hospitalization had received thromboprophylaxis, and a patient with pancreatic cancer and prior PE was not on secondary prevention. In contrast, other events occurred in settings where guideline-based prophylaxis was not formally indicated (e.g., ambulatory cancer patients with low Khorana score, acute bone fracture, or retrospectively diagnosed APS). These observations likely reflect a combination of therapeutic caution due to perceived bleeding risk and gaps in adherence to prophylactic recommendations. Reluctance likely stems from the perception of HHT patients as exclusively bleeding-prone. This is particularly important if one considers that patients with HHT often require hospitalization. In our cohort of 315 HHT patients, there were 154 hospitalizations during follow-up. Of these, 58 were due to emergency situations and 96 were planned hospitalizations for the execution of diagnostic and/or therapeutic procedures. Failing to use prophylaxis when indicated may contribute to the thrombotic burden in HHT, underscoring the importance of individualized risk–benefit assessment.
While some patients in our cohort received therapies potentially affecting thrombotic risk, all VTE events occurred in individuals not exposed to these agents, suggesting that the observed incidence is primarily related to HHT itself, the characteristics of the patients, or the management patterns during hospitalization.
Limitations of our study include the single center design, absence of a control group, and median follow-up shorter than the maximum observation period. We did not have access to a regional or national database to confirm capture of all VTE events. However, the nationwide referral nature of our center, structured follow-up, and cumulative observation exceeding 7,800 patient-months likely ensured identification of most events. Missed events would, if anything, underestimate rather than overestimate the true incidence. Additional potential biases include modest male predominance, a higher prevalence of pulmonary AVMs, older age, and chronic iron deficiency anemia—all factors that may increase VTE risk and reflect referral of more severely affected patients. We also did not retrospectively collect data on hospitalizations occurring in the year prior to study inclusion, and therefore cannot determine whether patients were hospitalized during that period. However, the four unprovoked VTE events occurred after 8, 10, 12, and 42 months of prospective follow-up, making a temporal link with prior hospitalization unlikely.
In conclusion, HHT patients appear to face a higher risk of VTE than the general population. Recognition of this thrombotic component is essential for personalized care in a disease classically defined by bleeding. Future strategies should integrate both hemorrhagic and thrombotic risks to guide comprehensive management.

Comments (0)