In our study, we observed a recurrent stroke rate of 0.70 per 100 person-years and TIA rate of 1.54 per 100 person-years after PFO closure. In patients with a recurrent event, there was a higher prevalence of hypertension. Furthermore, there was a trend towards a lower RoPE score. However, this was not significant.
To our knowledge, only a few studies investigated the clinical outcomes after PFO closure outside RCTs [16, 18,19,20,21,22]. These RCTs have shown low recurrent stroke rates after PFO closure, with a pooled incidence rate of 0.47 per 100-person years [13, 14]. Our study shows slightly higher recurrence rates than the RCTs. A potential cause can be the fact that RCTs have strict eligibility criteria, whereas observational studies investigate routine clinical practice. To illustrate, we included patients with TIA as an index event and patients above 60 years of age, if other criteria suggestive of a PFO-associated neurological event were present. Those patients were excluded from most RCTs.
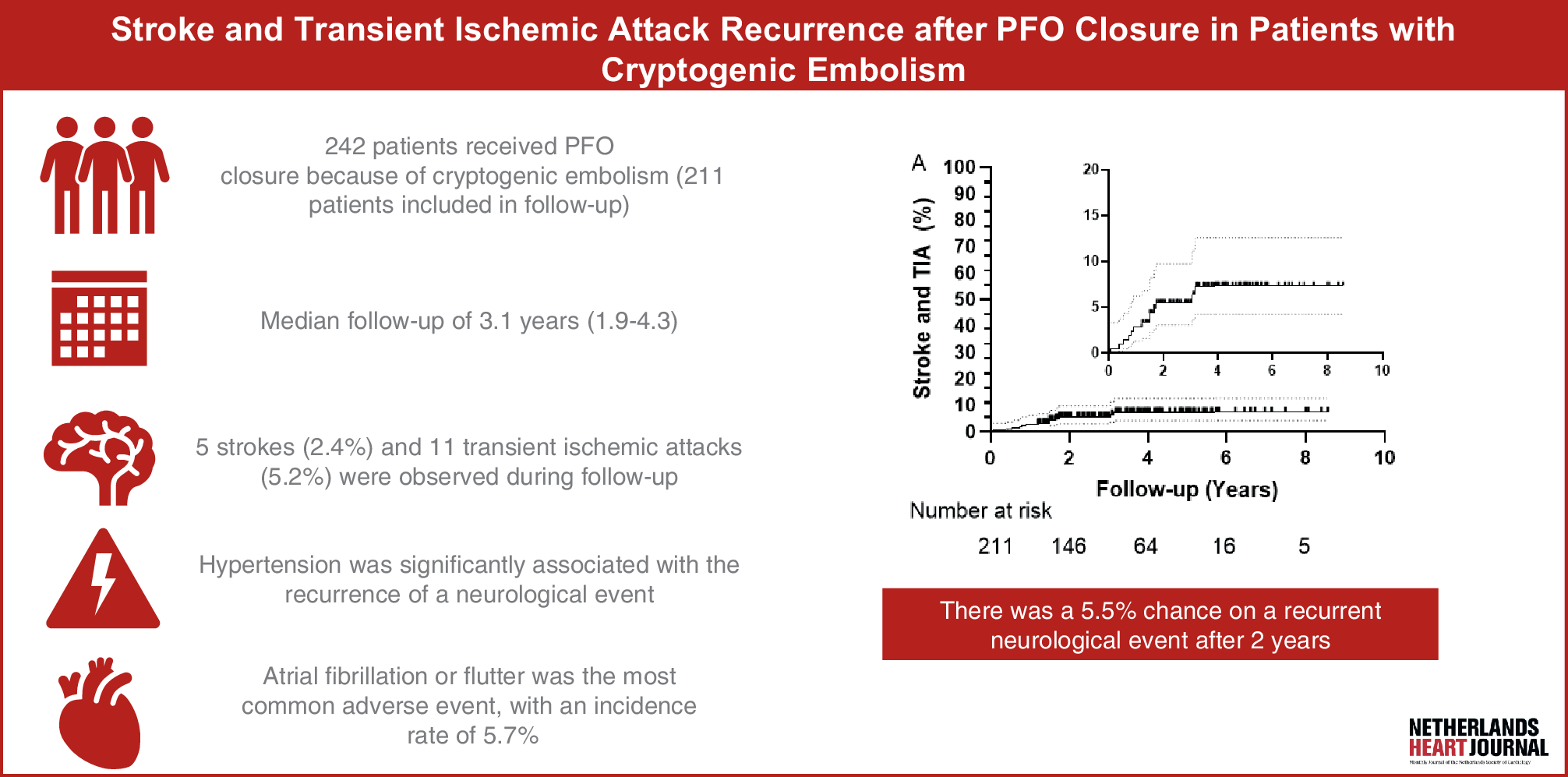
The combined recurrent stroke/TIA rate (2.24 per 100-person years) in our study is also higher compared to other studies. With a mean RoPE score of 7.2, a 6% chance of a recurrent neurological event in 2 years was expected with medical therapy, as estimated by the publication of Kent et al. [23]. Our Kaplan-Meier estimate shows a 5.5% chance of recurrent neurological events after 2 years in our cohort. When analysed separately, the estimated 2‑year risk was 1.5% for stroke and 4.5% for TIA. The 2‑year stroke risk in our cohort aligns with findings from a meta-analysis, including all major RCTs [13]. This suggests that the higher risk of recurrent neurological events in our cohort is mainly attributable to the higher risk of TIA. The meta-analysis showed no significant reduction in TIA risk after PFO closure compared with antiplatelet therapy [13]. Due to its transient nature, lack of biomarkers, and the overlap of clinical presentation with other conditions such as migraine, accurately diagnosing a TIA can be challenging [24]. With this in mind, it is reasonable to consider that the recurrent TIAs observed in our study may, in fact, represent another diagnosis, despite thorough neurological evaluation by a neurologist.
In our study, hypertension was significantly associated with the recurrence of a neurological event. This finding aligns with the study of Sørensen et al. [22] As also stated by Goessinger et al. [20], age accounts for 50% of the total RoPE score, whereas other individual risk factors only account for 10%. While the RoPE score provides valuable risk stratification, it may underemphasize the importance of individual cardiovascular risk factors, such as hypertension, and overemphasize the influence of age. Furthermore, the RoPE score does not include high-risk PFO features, like a large shunt or the presence of an ASA, which studies have demonstrated to be associated with an increased risk of recurrent stroke [15, 25]. We suggest that greater emphasis should be placed on evaluating individual, circumstantial, and anatomical risk factors, rather than relying exclusively on the total RoPE score. The PASCAL score, which includes anatomical risk factors and the ROPE score, is therefore now widely used in decision-making [14]. Moreover, strict control and monitoring of cardiovascular risk factors seem essential for secondary stroke prevention after PFO closure.
For patients above 60 years old, no clear recommendations are given in guidelines, as most RCTs excluded elderly patients. In our study, the rate of recurrent stroke/TIA did not differ significantly between patients aged below and above 60 years. This aligns with previous studies [20, 26]. We suggest that PFO closure may be safe for carefully selected patients over 60 years old and without cardiovascular risk factors, especially when high-risk PFO features are present. However, future RCTs are needed to prove this hypothesis.
Our study shows great safety of PFO closure in terms of periprocedural complications. Long-term complications of PFO closure were mainly AF or atrial flutter, which was seen in 12 patients (5.7%). This number is comparable to other studies, although incidence numbers differ slightly between different devices (4.7–7.6%). [5, 27,28,29] 8 out of 12 patients developed AF or atrial flutter within 45 days after the procedure, of which only one was persistent. Although this is not classified as a periprocedural complication, it strongly suggests an association with the procedure. These findings support the idea that AF after PFO closure tends to be transient, and the long-term risk of AF appears to be low [30].
Limitations
Our study has several limitations. First, a relatively large group of patients was lost to follow-up. Secondly, only major bleedings during follow-up are documented. Minor bleedings, therefore, could be missed, and the total amount of bleedings can be underestimated. Thirdly, due to the fact that primary outcomes and adverse events are infrequent, subgroup analyses are small. However, our study is one of the few studies providing real-world data on the recurrence of neurological events after PFO closure. Large multicenter studies are needed to enable more robust and well-defined subgroup analysis. Finally, analysis of the PASCAL score was not possible, as its regular documentation began only recently in our hospital. However, its criteria have already been used for decision-making for a long time.

Comments (0)