In the sections above, we already outlined why MRR is the first and so far, only index that is specific for the microcirculation and independent of epicardial stenosis. It is also more accurate and reproducible than bolus-derived IMR and CFR, and continuous thermodilution has proven to be safe [18]. On top of that, when both resting flow and resistance are measured and can be compared to hyperemic flow and resistance, it becomes possible to distinguish between functional and structural abnormalities of the microcirculation in a patient. Functional CMD due to endothelial dysfunction with impaired vasodilatory response results in elevated resting blood flow (Q) and decreased microvascular resistance (Rµ) at rest, but normal values at hyperemia. Structural CMD, on the other hand, is reflected by decreased hyperemic blood flow (Q) and increased hyperemic resistance (Rµ) [19]. This subdivision is important for understanding and diagnosing pathological disorders of the microcirculation, but especially for future research and development of better therapies for ANOCA patients. We have come a long way since ANOCA was poorly understood, referred to as ‘Syndrome X’ or over 20 different definitions, resulting in a very heterogeneous group of patients, which made it nearly impossible to develop treatment or good clinical guidelines for all of these patients. With the present armamentarium of physiological indices, this has changed dramatically. Although at this point it should be emphasized that MRR can theoretically also be calculated by using bolus thermodilution techniques, the strength of any device is not stronger than its weakest link. MRR calculated in such a way is, by definition, suboptimal compared to MRR calculated by absolute flow measurements. In addition, without absolute flow measurements, no quantitative value of Q (in ml/min) and Rµ (in WU) are available, and the distinction between functional and structural microvascular disease remains difficult. Therefore, using absolute flow measurements and continuous thermodilution remains preferable for optimal assessment of the coronary microcirculation.
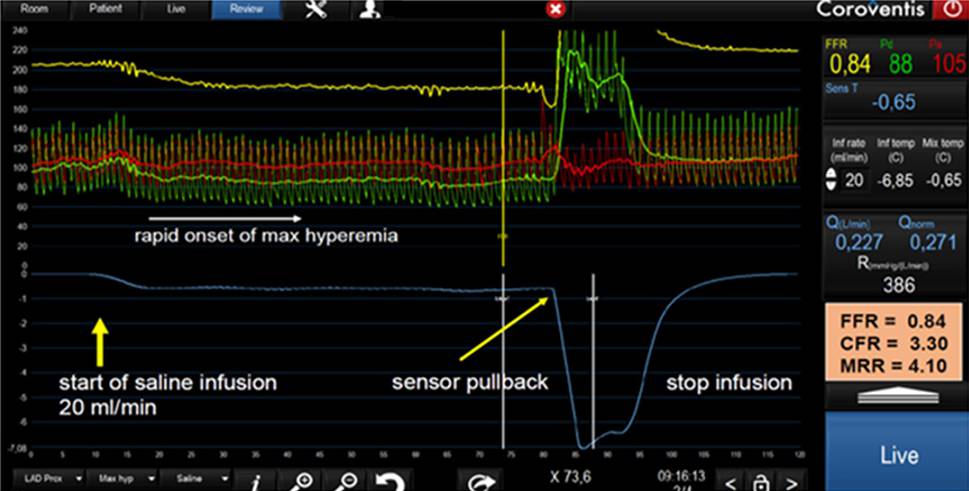
For the implementation of absolute flow and resistance measurements and MRR in the cathlab some specific equipments are required. For cathlabs already performing bolus thermodilution in CFT, most materials will be present already, such as the pressure wire, high-pressure infusion pump, and Coroventis software. However, the dedicated Rayflow ®infusion catheter (Hexacath, Paris) is mandatory for a complete and homogenous mixture in the investigated artery. It should also be stressed that a high-pressure infusion pump should be used for saline infusion, like a contrast injector is used in left ventricular angiography. Such a pump should be programmed in the infusion mode (ml/min) and not in its injector mode (ml/sec). Although the technique is very easy to learn, some centres will find the cost of the necessary equipment, as well as being unfamiliar with the measurements, an impediment to starting to measure absolute coronary blood flow and microvascular resistance by continuous thermodilution. It is understandable that any new index needs time before growing from pioneering to becoming a tool being fully adopted in daily practice, as was the case with FFR. There is now a small but expanding body of evidence showing the accuracy and added value of MRR, and this will lead to cardiologists becoming more and more accustomed to these parameters.
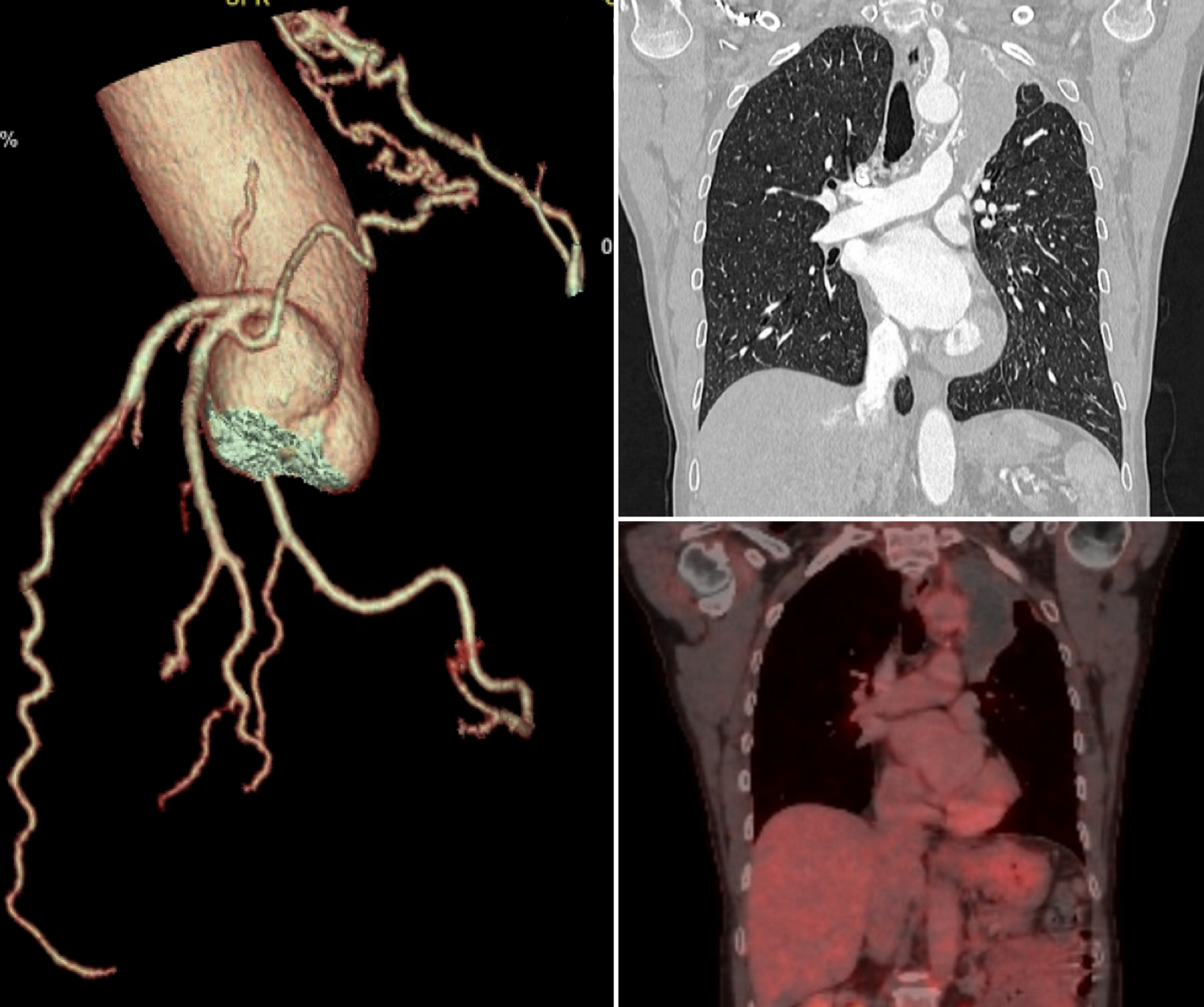
Outside of the cathlab, MRR can be approximated as well. The equation showing that MRR = CFR/FFR × Pa,rest/Pa,hyp, illustrates that non-invasively obtained measurements of CFR and FFR by CT and PET can also be used to calculate MRR, if at least Pa at rest and hyperemia are carefully measured non-invasively during PET. Further developments in measuring MRR by combined parameters, for instance, CT-derived FFR and CFR from PET-CT are being investigated. One should realise, however, that a complete Coronary Function Test also contains Acetylcholine-based testing for epicardial coronary spasm. Unfortunately, that diagnostic part of CFT is difficult to acquire in a non-invasive manner.
Indices with one true cut-off point between ‘health and disease’ are rare in clinical medicine. For example, FFR equals ∿ 1.0 in every normal patient and every normal coronary artery. Therefore, a sharp cut-off value for FFR can be expected (around 0.8) with minimal grey zone. MRR shares the disadvantage with CFR to be age-dependent and shows some heterogeneity. Therefore, by definition, a grey zone exists between strictly normal and abnormal values. Presently available data suggest that with MRR-values above 3.0, microvascular disease can be excluded and that below a value of 2.3, microvascular disease is likely to be present [20, 21]. We expect further research to identify the correct boundaries for MRR in diagnosing microvascular dysfunction.

Comments (0)