This study is part of a quality improvement project, conducted by the PCI registration committee of the Netherlands Heart Registration (NHR), in close collaboration with the Dutch Association of Health Insurers (in Dutch: Zorgverzekeraars Nederland) and the Dutch Health Care Information Centre (Vektis). Within the NHR, cardiologists and cardiothoracic surgeons register baseline, procedural, and outcome data for all invasive cardiac interventional, electrophysiological, and surgical procedures. Through public reporting, the NHR provides transparency of outcome data to cardiac patients, healthcare providers, and policymakers [15]. The interpretation of the registered data is primarily managed by registration committees, where designated cardiologists and cardiothoracic surgeons represent their hospitals. When relevant variations in outcomes are observed, the committees discuss healthcare delivery processes and share best practices. Additionally, these registration committees conduct quality improvement projects, including this study.
Data source
This retrospective observational cohort study utilized data from a nationwide all-payer claims database managed by Vektis, containing medical care claims reimbursed by Dutch national insurance companies. Since 99.9% of the Dutch population has health insurance [16], this database almost covers all medical care provided to the Dutch population. This study obtained claims data on lipid-lowering medication prescriptions for patients undergoing either elective PCI (health care activities 33231-33234) or acute PCI (health care activity 33238) from the Vektis database.
Study population
This study included all patients undergoing acute or elective PCI from January 1, 2018, to December 31, 2020, in the Netherlands. Patients who died within 365 days post-PCI were excluded, and in cases of multiple PCIs within a calendar year, only the first PCI was included.
Lipid-lowering treatment and adherence
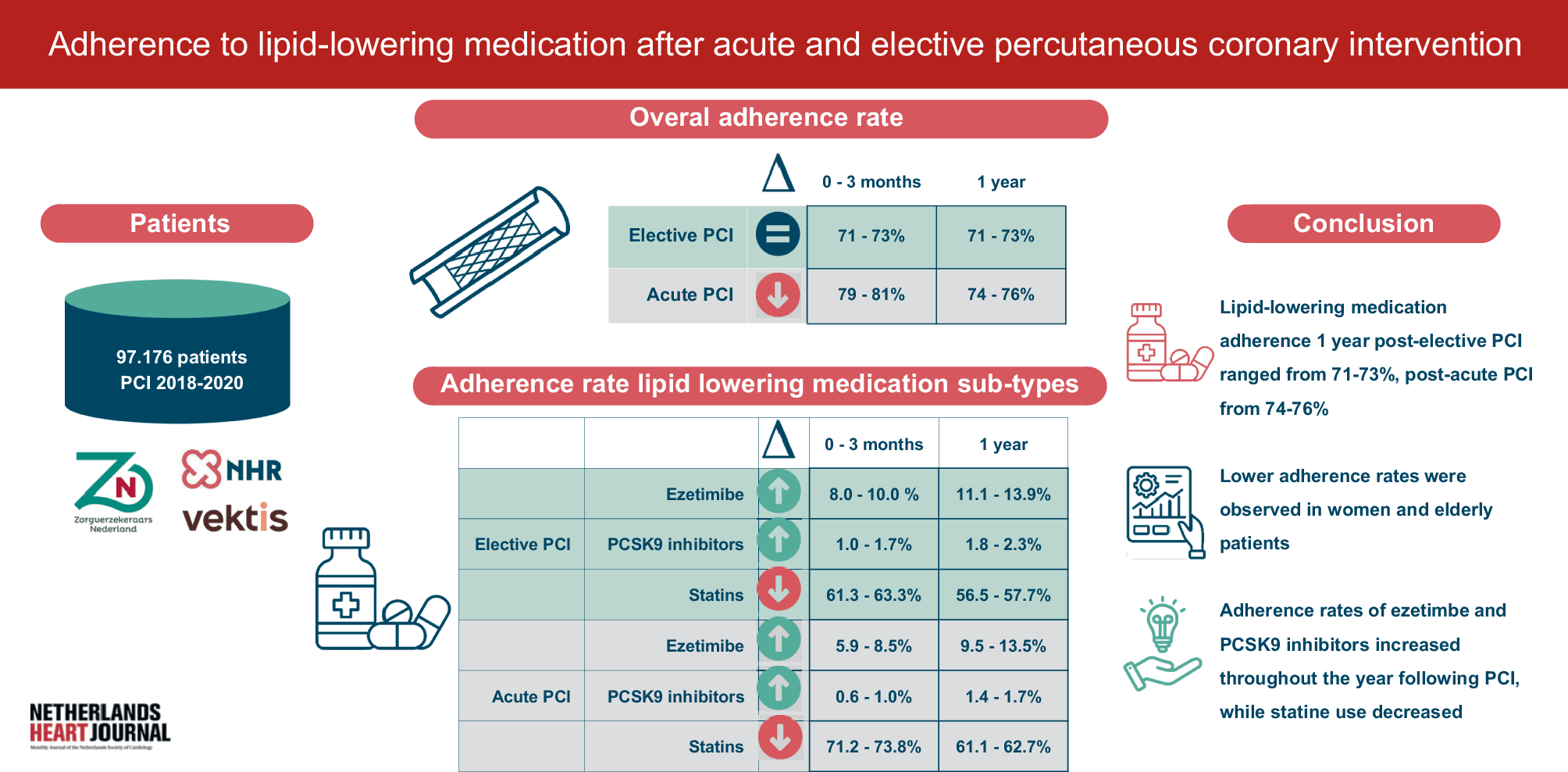
We utilized the Vektis registry to extract data on whether patients were dispensed lipid-lowering medication at the pharmacy, using Anatomical Therapeutic Chemical (ATC) codes, and to ascertain the duration of the active lipid-lowering medication prescription. We extracted data on whether patients had been prescribed statins (ATC code C10AA01, C10AA03, C10AA04, C10AA05, and C10AA07), ezetimibe (ATC code C10AX09), and/or PCSK9 inhibitor (ATC code C10AX13 or C10AX14) dispensed at the pharmacy 90-1 days prior to PCI, and 1–365days after PCI.
Adherence to lipid-lowering medication was assessed at baseline until one-year post-PCI, defined as a medication possession rate (MPR) ≥ 80% during a specified period. Patients with an active lipid-lowering medication prescription and an MPR below 80% were considered non-adherent. Patients without an active prescription (MPR = 0%) were defined as non-users. A cut-off value of 80% was chosen as this is in line with existing literature [17], and because we aimed to include those patients who used the lipid-lowering medication with a reasonable dosage, while avoiding that patients are wrongly excluded because of administrative mistakes. Patients adherent to lipid-lowering medication were divided into three groups: those prescribed statins, ezetimibe, or PCSK9 inhibitors. We used the most recent prescription in each period to categorize patients. If multiple categories of lipid-lowering medication were dispensed on the same day, categorization followed this order: (1) PCSK9 inhibitors, (2) ezetimibe, and (3) statins. Additionally, we assessed the distribution of adherence rates among different statins subtypes and described trends in prescription behaviour from 2018–2020.
Statistical methods
Discrete variables were presented as numbers and percentages, and normally distributed continuous variables as mean ± standard deviation (SD). Baseline adherence was evaluated during the three months prior to PCI. For patients who initiated lipid-lowering medication during this period, MPR was calculated from the first dispense date until the PCI date. Adherence rates for lipid-lowering medication were then assessed over the year following PCI, divided into four three-month periods (0–3, 4–6, 7–9, and 10–12 months post-PCI), and reported separately for 2018, 2019, and 2020 to monitor trends. The period 0–3 months post-PCI was referred to as initial adherence, and 10–12 months as long-term adherence. Adherence rates for lipid-lowering medication subtypes (statins, ezetimibe, and PCSK9 inhibitors) and statin subtypes (simvastatin, atorvastatin, rosuvastatin, and others) were also specified. Secondary analyses stratified lipid-lowering medication adherence rates by sex and age to examine differences in sex and adherence rates between patients aged 80 years and older versus patients younger than 80 years. We also performed subgroup analyses for the patients with single PCI and the patients with a recurrent PCI within 1 year. A sensitivity analysis was performed for the patients who died during follow-up.
Additionally, long-term adherence rates for lipid-lowering medication were reported for individual PCI centres to assess clinical practice variations. To mitigate yearly variation effects, data from 2018, 2019, and 2020 were combined for both elective and acute PCI cases. We also classified the PCI centres into regions (i.e., Northern, Eastern, Western, and Southern Netherlands) and into SES-WOA score regions (i.e., score < 0.0 and ≥ 0.0). SES-WOA concern the socioeconomic scores of private households, which are calculated by Statistics Netherlands (CBS) and based on household data concerning welfare (a combination of income and wealth), highest level of education and recent labour participation. To classify the hospitals into categories, we used the geographical map of the Dutch Ministry of Health, Welfare and Sport [18].
All statistics were computed using SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA).

Comments (0)