This multicenter NHR study examined ablation strategies in patients with durably isolated PVs undergoing repeat AF ablation. A wide range of strategies is being used, with posterior wall ablation being the most common. However, no significant differences in arrhythmia recurrence were observed between strategies, including no additional ablation, regardless of AF type (paroxysmal or persistent).
Incidence of durably isolated PVs during repeat AF ablation
Previous studies have shown a variable incidence of durably isolated PVs in patients with AF recurrence presenting for repeat AF ablation, with reported rates ranging from 15–40%, depending on patient population, operator expertise, and ablation technique [1, 10,11,12]. The percentage of patients with isolated pulmonary veins is slightly lower than previously reported in the literature. Our data is based on a real-world registry in which ablation was performed using various techniques by a broad range of operators with differing levels of experience. This may explain the discrepancy compared to other studies, which were often conducted in expert centers, either within or outside the framework of standardized ablation protocols—for example, as part of a multicenter randomized controlled trial.
The incidence of durable PVI increases with the number of previous PVI procedures [17, 18]. A sub-analysis of the FIRE AND ICE trial examining findings at repeat ablation procedures indicated a higher incidence of durably isolated PVs following cryoballoon compared to radiofrequency ablation (21.9% vs. 17.3%) [19]. However, a recent study by De Potter et al. reported a much higher incidence of 62% after index ablation using CLOSE-guided ablation, which involves precise delivery of contact-force guided point-by-point radiofrequency ablation [11]. Emerging technologies, such as pulsed field ablation, may further improve lesion durability [20]. Data from two recently published large multicenter registries, the EU-PORIA registry and the MANIFEST registry, observed that 38% and 45.5% of patients, respectively, had durably isolated PVs at repeat ablation after initial PVI with pulsed field ablation [21, 22]. Considering this is a first-generation technology, with the improvement and development of novel ablation technologies and strategies, the number of patients with durably isolated PVs during repeat procedures is likely to increase.
Current ablation practices in patients with durably isolated PVs
The presence of durably isolated PVs in many patients with recurrent AF suggests that arrhythmogenic sources lie outside the PVs. While extra-PV ablation strategies have shown benefits in select subgroups, no single approach has proven superior to PVI. This uncertainty explains the lack of consensus on the best ablation strategy for treating these patients, suggesting that an individualized approach may be necessary.
In the recent retrospective PARTY-PVI study, Benali et al. compared various ablation strategies during repeat ablation for AF in 367 patients with durably isolated PVs from 39 centers [10]. Most patients were males (67%) with persistent AF recurrence (56.4%). Only one ablation strategy (54.5%) was commonly used, followed by two or three (37.1% and 6.5%). Similar to our findings, they observed no significant difference in AF-free survival across strategies, with LA size being the only independent predictor of recurrence. Notably, Benali et al. grouped similar strategies to boost statistical power, but did not assess the effects of individual strategies, report the overall incidence of durably isolated PVs, or specify how many patients received no additional ablation. Ackmann et al. reported a similar analysis using a contemporary ablation cohort. Durable PVI was observed during remapping in only 20.1% [13]. A range of ablation strategies was employed in patients who presented with isolated pulmonary veins. They also demonstrate that no specific ablation approach yields superior outcomes over another.
Recently, preliminary findings from the ASTRO-AF study were presented [14]. This multicenter, prospective, randomized study compared substrate modification and left atrial appendage isolation in 161 patients with durably isolated PVs [14]. They found no statistically significant difference in AF/AT recurrence at one year between the two ablation strategies. Of note, more than half of the patients had undergone more than one prior ablation procedure. Due to futility, the study was prematurely terminated after randomizing 63% of the planned patient population.
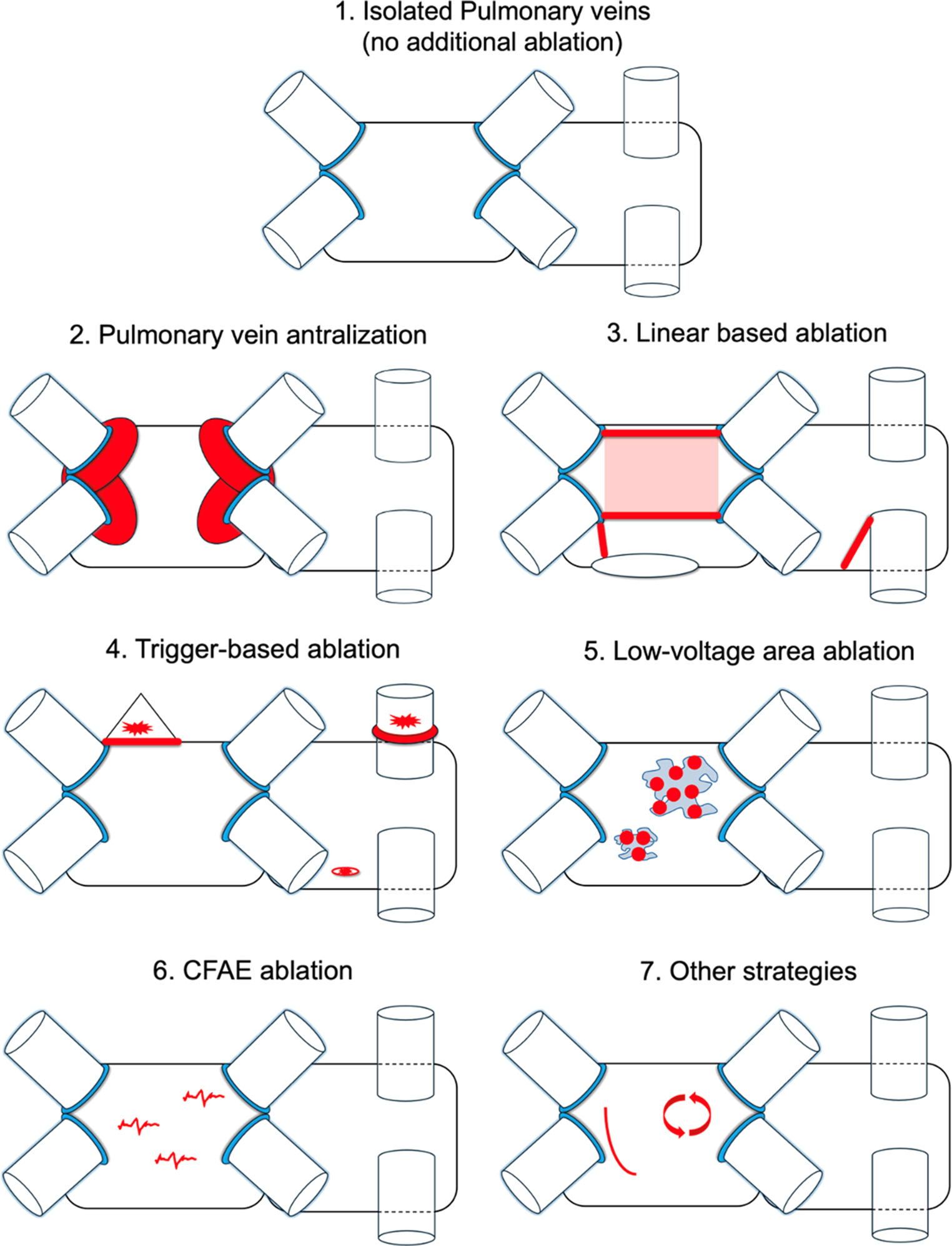
In our study, posterior wall isolation was the predominant strategy (58.4%) employed in patients with durably isolated PVs. The posterior wall is widely accepted as a major extra-PV harbor for AF triggers and drivers, partly attributed to the shared embryological development with the PVs [23, 24]. However, conclusive evidence regarding its efficacy beyond PVI alone remains inconsistent and inconclusive, with currently available data showing contrasting results [25, 26].
Few studies have assessed outcomes of repeat ablation in patients with durably isolated PVs. In our cohort, atrial arrhythmia recurred in 52.8% of patients. The PARTY-PVI study by Benali et al. reported a 43.3% recurrence rate at two years, with no significant differences between various ablation strategies or their combinations [10]. Similarly, the ASTRO-AF study found one-year recurrence rates of 48.3% for low-voltage area ablation and 44.5% for empirical left atrial appendage isolation, again with no significant difference [14]. De Pooter et al. observed a 39% recurrence rate at one year using empirical trigger ablation (e.g., superior vena cava isolation or PV antralization) and substrate ablation (linear lesions at the roof, mitral isthmus, or anterior wall) [11]. A small single-center series reported comparable outcomes using diverse approaches such as extra-pulmonary trigger ablation, CFAE ablation, and linear lesions [27, 28]. Unlike our study, none of these investigations included a control group of patients who underwent no additional re-ablation.
Our study, like others, shows that outcomes of AF ablation in the setting of isolated pulmonary veins are suboptimal, and no conclusions can be drawn regarding a preferred ablation strategy. Future studies are needed to provide more clarity, starting with the use of pulsed-field ablation (PFA). Evidence for the optimal strategy should come from a well-powered multicenter randomized controlled trial. Potential approaches may include ablation guided by high-density (functional) substrate mapping [29, 30]. Promising new techniques, such as spatiotemporal dispersion ablation [31], also warrant further investigation.
Limitations
The main limitation of the current study is that it is an observational study. There was no control group, and the study was not randomized. Also, our study is subject to selection bias, as the strategy and choice to perform additional ablation were determined by the operator at the time of the procedure In addition, detailed procedural data, such as ablation settings and exact ablation locations, were unavailable, and the execution of ablation strategies is operator dependent. This limits the ability to assess strategy-specific effects.
AF recurrence detection was not standardized, possibly underestimating recurrence; nevertheless, recurrence rates were high, suggesting that AF recurrence is very common in this subset of patients.
Pulsed field ablation was not yet utilized in the current analysis. It is possible that if PFA had been used as the ablation technique instead of radiofrequency, the outcome of the analysis might have been different. It should be emphazised that identification of these patients is only possible during repeat procedures, making large-scale inclusion difficult. Nonetheless, through the NHR, we identified one of the largest cohorts of patients with durably isolated PVs.

Comments (0)