
Remember me
This was a prospective, single-centre, observational study conducted on the cardiology wards of the Amsterdam University Medical Centre (AUMC). Patient enrolment took place between March 2024 and April 2025. The study was approved by the local ethics committee, and all participants provided written informed consent.
A convenience sample of 25 participants was selected. This small sample size and exploratory design were chosen specifically to perform feasibility testing of the UPG device and to obtain initial data estimates necessary for hypothesis generation and the power calculation of the future adequately sized randomised controlled trials. As the primary objective was to assess the technical accuracy of the UPG, which is attached non-invasively to the urine collection bag, long-term clinical outcomes, such as catheter-associated urinary complications, were not recorded.
Study populationEligible patients were ≥ 18 years of age, admitted to the cardiology wards with an indwelling urinary catheter for standard clinical monitoring prior to study enrolment, and able to provide informed consent. Exclusion criteria were chronic anuria, known urological disorders, catheter dysfunction, anticipated catheter removal during the observation period, or a urine production rate of < 30 mL/h.
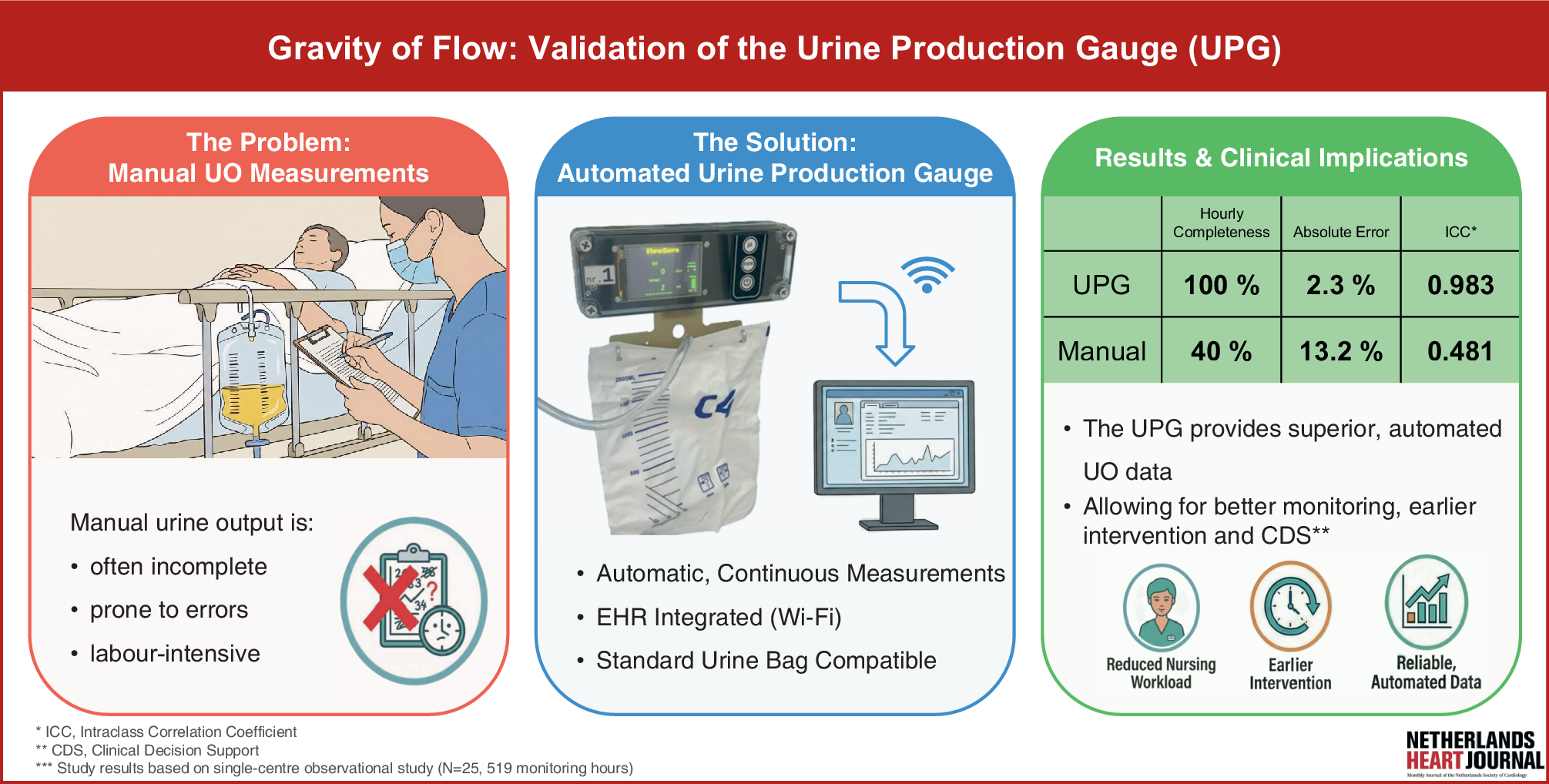
Urine production gaugeThe UPG is a reusable, in-house-developed device that measures urine production by tracking catheter bag weight over time using a load cell (Fig. 1). It features an integrated rechargeable battery and transmits measurements over Wi-Fi to the Electronic Health Record (EHR) through a custom HL7 server; the microcontroller includes a proprietary motion-artifact algorithm to filter noise and ensure stable, continuous measurements. As an in-house developed device, it currently has no CE mark and may be used only in approved clinical research.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.The data transfer architecture was co-designed with an application architect and approved by internal governance. A data privacy impact assessment confirmed that privacy risks are adequately mitigated, and security measures ensure the protected transmission of the data.
Preclinical validation used a two-point calibration with infusion fluid (empty bag and 2 L), from which the calibration factor was derived. Linearity was confirmed with fixed weights, and functionality was tested by simulating urine production at varying infusion rates. As the load cell responds proportionally to any liquid, calibration with infusion fluid is appropriate. Given normal urinary specific gravity (1.003–1.030), applying a 1 g ≈ 1 ml conversion yields a clinically acceptable estimate, with a potential error margin of ~3% [5, 6].
Measurement procedureFor each participant, urine output was recorded manually using a conventional manual urinometer (MU) and automatically with the UPG. Nurses documented the manually measured volume and timestamps on a worksheet, while the UPG logged data continuously. Observation periods lasted 8–24 h, during which all urine was drained into a 24-hour reference container serving as the gold standard for cumulative output.
At the start of each observation, collection bags were emptied, attached to the UPG, and nurses who had undergone group training were re-instructed on the study protocol at the start of each observation period and were instructed to brief their colleagues during subsequent shifts. A device manual was available on the ward.
Participation did not alter patient care. Patients could mobilise freely, and the catheter bag could be temporarily disconnected without affecting the study. The system detected weight absence during disconnection and, once reattached, computed the delta in urine volume, ensuring accurate output regardless of mobility.
Outcome measuresThe primary outcomes were (1) the completeness of hourly urine output registration, defined as the proportion of planned hourly measurements successfully captured by each method over a maximum of 24 h, and (2) the accuracy of cumulative urine output, determined by comparing volumes obtained with the MU and the UPG against the 24-hour reference standard.
Statistical analysisDescriptive statistics are reported as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate. Completeness between UPG and manual documentation was compared using the Wilcoxon signed-rank test for paired samples. Completeness by shift was assessed with the same approach. Agreement between each method’s volume measurements and the gold standard was evaluated using Bland–Altman analysis, reporting bias, and 95% limits of agreement.
Accuracy was further assessed using absolute and signed percentage errors. Reliability was quantified using intraclass correlation coefficients (ICC) with 95% confidence intervals. Equivalence of UPG and manual methods against the gold standard was tested using two one-sided tests (TOST) within a ± 5% predefined margin. Subgroup analyses across strata of 24-hour urine volume (< 1000, 1000–2000, > 2000 mL/24 h) were limited to descriptive statistics, as group sizes were small and the study was not powered for inferential comparisons. Median values and interquartile ranges were reported for each subgroup. All analyses were performed in Python (version 3.13, PyCharm environment). Two-sided p-values < 0.05 were considered statistically significant.
Comments (0)