
Remember me
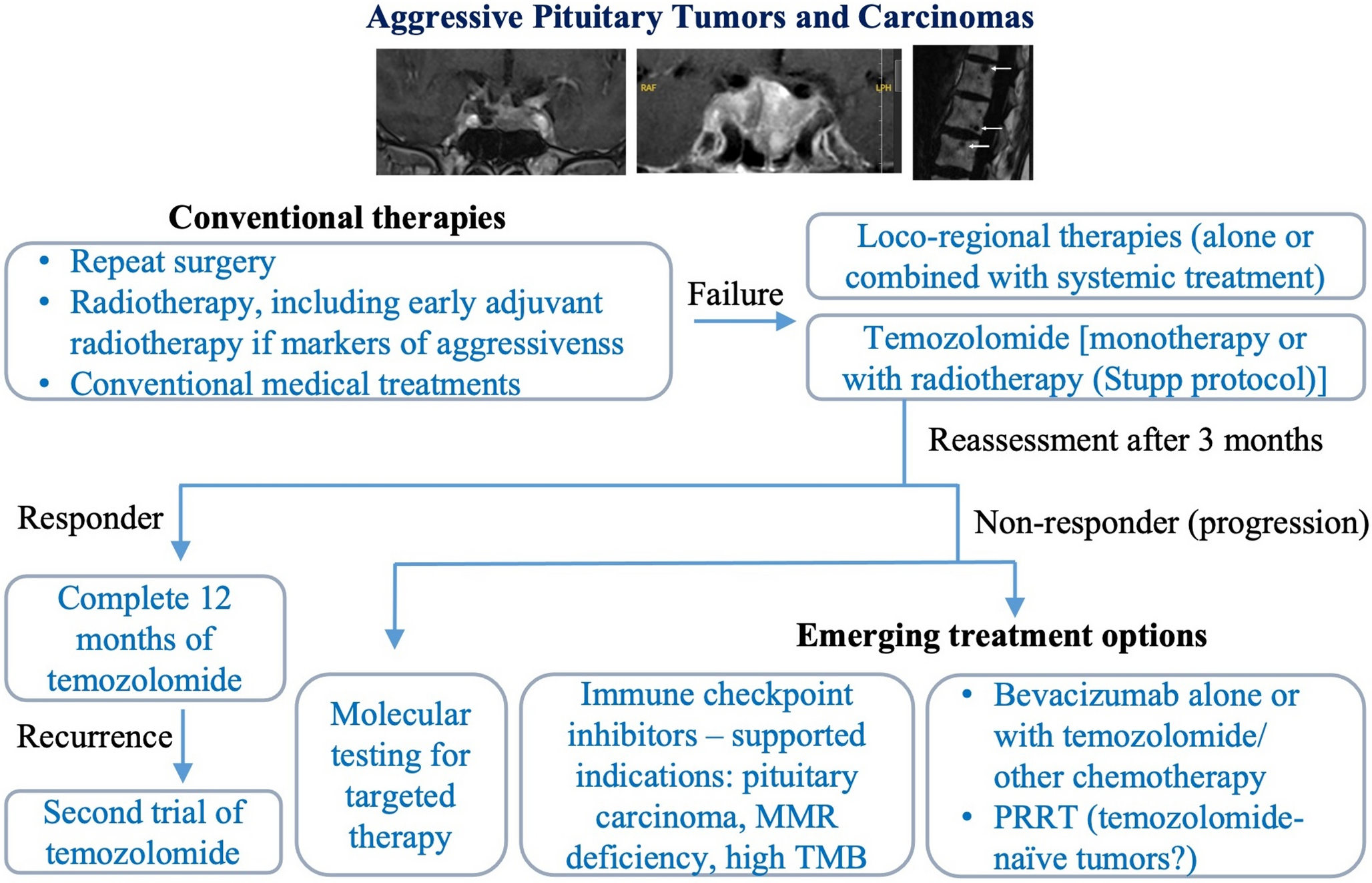
After temozolomide failure, the initial guidelines suggested a trial with other systemic cytotoxic therapy. However, given the variety of chemotherapeutic agents that had been reported and the lack of evidence, they were unable to suggest a particular regimen at that time [12]. Since, more data has accumulated which led to significant changes in the revised guidelines [1], as discussed below.
3.1 Molecular-guided druggable targetsFirst, to guide potential treatment choices, the revised guidelines suggest molecular testing in patients with tumor progression on temozolomide [1]. This molecular testing may provide information on specific gene alterations that can be targeted therapeutically, but also additional information, such as the tumor mutational burden and the mismatch repair deficiency status, for example [1].
Regarding the utility of molecular profiling in aggressive pituitary tumors and carcinomas, in a recent study, Paes et al. sequenced a cohort of 20 patients with prolactinomas to identify somatic genetic alterations. By doing so, they identified a somatic activating mutation in the estrogen receptor alpha gene in a patient with an aggressive lactotroph tumor resistant to temozolomide. This led to treatment with elacestrant, a second-line estrogen-receptor degrader. Elacestran was initiated after the third course of radiotherapy was completed and managed to significantly reduce prolactin levels and to control tumor growth for the available follow-up [23].
Another important point is that the respective somatic mutation, while present on the tissue sample from the fourth surgery, it was absent on the tissue samples from the first and second surgeries [23], underlying the need of a recent tissue sample for molecular profiling. In addition, Lin et al. demonstrated that different lesions from a same patients may harbor different molecular profiles, that may influence the response to treatment, more specifically to ICIs in the respective study [21].
In line with this, in the revised guidelines, it is noted that performing genomic analysis on recent tumor tissue is important, and hence to consider minimal invasive surgical biopsy as it poses minimal risk [1]. Having tissue available from different tumor sites in the case of pituitary carcinomas appears equally important.
3.2 ImmunotherapySecond, among emerging treatment options, ICIs have gained the most attention in recent years. The revised guidelines suggest considering a trial with ICIs in patients with pituitary carcinoma and rapid tumor progression after treatment with temozolomide. They also note that tumor agnostic data supports the use of ICIs in tumors that are either mismatch repair deficient or exhibit high tumor mutational burden, supporting the use in pituitary tumors with these molecular features [1].
By blocking immune checkpoints, “the brakes” of the immune system, ICIs reactivate and enhance anti-tumoral immune responses [24]. More specifically, ICIs used so far for the treatment of pituitary tumors block cytotoxic T-lymphocyte-associated protein (CTLA4) in the case of ipilimumab, and programmed cell death protein 1 (PD-1) in the case of nivolumab and pembrolizumab [10]. These molecules were used either as combined therapy (nivolumab + ipilimumab) or as monotherapy – usually pembrolizumab, but nivolumab monotherapy was also used [10].
The tumor response of 38 pituitary cases has so far been reported. These cases come from a cohort of 15 cases [25], a phase 2 clinical trial of nine cases [21], another phase 2 clinical trial of four cases [26], while the others are cases from the second European Society of Endocrinology survey [4] or from isolated case reports [11, 22, 27,28,29,30,31,32]. All 38 patients received multimodal treatment before ICI start, including temozolomide in at least 36 cases [4, 11, 21, 22, 25,26,27,28,29,30,31,32].
Under ICIs, complete response was noted in one case (2.6%) [32], partial response in nine cases (23.6%), stable disease in nine cases (23.6%), while 19 (half) of the tumors progressed [4, 11, 21, 22, 25,26,27,28,29,30,31,32] (Fig. 1). Figure 1 shows the tumor response for all cases, while Fig. 2a the response separately for pituitary carcinomas versus aggressive pituitary tumors, and Fig. 2b the response separately for dual therapy versus monotherapy with pembrolizumab. However, as with all treatments, one should bear in mind that different studies or case reports have evaluated differently the tumor response, and that the duration of the response is also variable [4, 11, 21, 22, 25,26,27,28,29,30,31,32].
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Tumor response in aggressive pituitary tumors and carcinomas. Abbreviations: immune-checkpoint inhibitors (ICIs), bevacizumab (BVZ), peptide receptor radionuclide therapy (PRRT), complete response (CR), partial response (PR), stable disease (SD), progressive disease (PD). Made with Graphpad Prism version 10.6.1
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Tumor response to immune-checkpoint inhibitors in aggressive pituitary tumors and carcinomas considered separately for pituitary carcinomas versus aggressive pituitary tumors (a), as well as separately for dual therapy versus monotherapy with pembrolizumab (b). Abbreviations: pituitary carcinomas (PCs), aggressive pituitary tumors (APTs), ipilimumab (IPI), nivolumab (NIVO), complete response (CR), partial response (PR), stable disease (SD), progressive disease (PD). Made with Graphpad Prism version 10.6.1
Regarding predictors of response to treatment, in our cohort study we identified that tumor type (i.e., pituitary carcinoma versus aggressive pituitary tumor) was a major predictor of response to ICIs, with pituitary carcinomas responding better. With the publication of more data, although this difference persists, it appears to become less pronounced (Fig. 2a).
As noted in the revised guidelines, mismatch repair deficiency and high tumor mutational burden are known predictors in other cancers [1]. Tumor mutational burden appears promising as a predictive factor of response in aggressive pituitary tumors and carcinomas, as well; however, it is noteworthy that a high tumor mutational burden has been associated with a favorable radiological response in most, but not all treated cases [4, 10, 11, 13, 21]. Similarly, although mismatch repair deficiency appears promising, not all mismatch repair-deficient cases responded to ICIs [10, 21].
Regarding the histological type, the cases treated consist of 24 corticotroph tumors, 12 lactotroph tumors, one Pit1 silent tumor and a somatotroph tumor [4, 11, 21, 22, 25,26,27,28,29,30,31,32]. One corticotroph tumor showed complete response, six (25%) partial response, three (12.5%) stable disease, while 14 (58.3%) progressed. On the other hand, two (16.7%) lactotroph tumors showed partial response, five (41.7%) stable disease, while the other five (41.7%) progressed. Thus, it is difficult to say whether tumor histological type might play a role.
Finally, only four patients with corticotroph tumors had hypercortisolism during ICIs administration [4, 10, 11, 21, 22, 25,26,27,28,29,30,31,32]. The numbers are too low to draw any definitive conclusion, nonetheless, given the immunomodulatory effect of glucocorticoids, it appears prudent to aim for eucortisolism.
Regarding immune-related adverse events, as reported also for other cancers, more frequent and more severe adverse events occurred when using combined immunotherapy versus monotherapy [4, 11, 21, 22, 25,26,27,
Comments (0)